


SERMs Vs Aromatase Inhibitors: PCT Estradiol Guide
In a corporate slide deck, "SERMs vs AIs" gets treated like a tidy toggle switch. Pick one, move on, recover. Real life is messier.
The clean, practical answer is this: in post-cycle therapy (PCT), a SERM is usually the main engine for restarting LH/FSH and natural testosterone production, while an aromatase inhibitor is a situational tool for documented high estradiol that is actively causing problems. If you flip that relationship, you can feel "controlled" for a week or two while your HPTA stays asleep.
Also, the usual disclaimer that somehow still matters: I'm not your clinician, and endocrine therapy is not a game. If you can involve a real endocrinology or men's health provider, do it.
What problem does each tool actually solve?
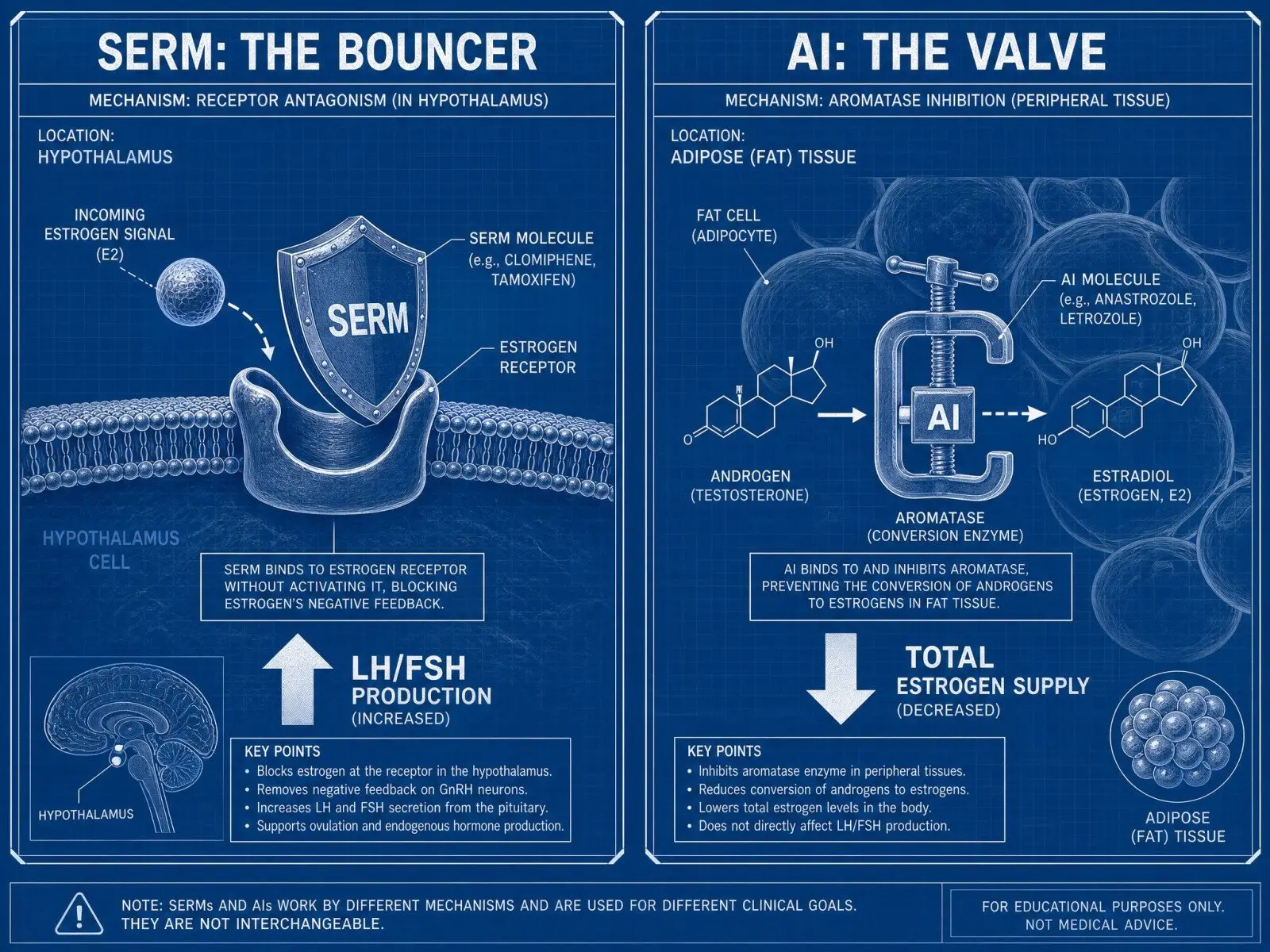
You'll hear "estrogen control" tossed around like it's one thing. It isn't. The body has estrogen receptors in different tissues, and it has estrogen production happening through the aromatase enzyme in multiple sites (fat tissue is a big one). SERMs and aromatase inhibitors target different choke points.
Receptor blockade
A Selective Estrogen Receptor Modulator (SERM) (tamoxifen, clomiphene, enclomiphene) plays bouncer at the estrogen receptor, especially in the hypothalamus and pituitary, so estrogen's "we're good here, stop signaling" feedback gets muffled. That matters in PCT because the whole point is to get gonadotropins moving again.
The more technical version, if you like mechanisms: SERMs act as tissue-selective agonists or antagonists at the estrogen receptor alpha and related receptor configurations, which is why they show up in breast cancer therapy and fertility medicine, not just gym lore. If you want the deep pharmacology, this breakdown of SERM signaling in the hypothalamic-pituitary axis is worth your time because it lays out why LH/FSH respond the way they do in men: how clomiphene and tamoxifen modulate gonadotropin release.
Aromatase inhibition
An aromatase inhibitor (anastrozole, exemestane, letrozole) targets the enzyme complex that converts androgens into estrogens. That means serum estradiol tends to drop, sometimes fast, sometimes too far. Exemestane is a steroidal, sometimes-described irreversible steroid inhibitor; anastrozole and letrozole are competitive inhibitors. In plain English: AIs change the supply, not the receptor's ability to "hear" the signal.
If you want a readable summary that doesn't pretend estrogen is evil, the explanation in this overview of estrogen blockers vs aromatase inhibitors lands the key distinction without overcomplicating it.
Non-interchangeable roles
The easiest way I've found to keep people from face-planting is to name the job, not the drug class.
- Restart job (HPTA): typically a SERM, because you're pushing hypothalamus-pituitary signals (LH/FSH).
- Overflow job (excess estrogen): sometimes an aromatase inhibitor, because you're reducing estrogen synthesis when levels are genuinely high and symptomatic.
- Local tissue flare job (gyno onset, nipple sensitivity): often SERM-leaning, because receptor activity in breast tissue matters even when your blood number is only "meh."
I'm blunt about this because I've watched the same mistake loop forever: people treat AIs and SERMs like interchangeable knobs, then act surprised when libido, mood, and recovery wobble. The framing in this discussion of AIs vs SERMs as separate tools matches the basic reality: they are solving different problems, in different places, through different mechanisms.
How does each choice change estradiol and feedback?

This is where the confusion gets expensive.
Serum E2 direction
AIs usually push estradiol levels down. SERMs often don't. They can even leave estrogen levels the same or higher, because blocking receptor feedback can lead to more upstream signaling and more aromatase activity downstream, depending on the context.
So if your entire plan is "I want lower E2," a SERM is a weird pick. If your plan is "I want my pituitary to stop acting like it's on vacation," a SERM suddenly makes sense.
Hypothalamus-pituitary signals
Post aas cycle, your hypothalamus and pituitary can be suppressed, and your testes might be under-stimulated. SERMs are used because they tend to increase LH/FSH. That's the "reboot layer," and I'm unapologetic about calling it that.
AIs can raise testosterone too, technically, because less aromatization can alter feedback and improve the testosterone/estradiol ratio. You can see that dynamic in clinical contexts where anastrozole increased testosterone in men with low T in a proof-of-concept trial: anastrozole vs testosterone gel outcomes. Useful data point, but it's not a blank check to run an inhibitor like it's candy.
Testosterone recovery effects
SERMs often create a "looks better on labs" bump, especially in total testosterone, because the axis is being whipped into signaling again. The catch is that feeling good depends on more than the number. Estradiol is part of male sexual function, endothelial health, mood stability, and joint comfort. Crush it and you can get erectile dysfunction, flat affect, creaky joints, and a weird sense that your body forgot how to recover.
There's also the side-effect reality. A survey analysis on performance drug users found meaningful differences in reported adverse events between SERMs and AIs, including mood changes and sexual side effects: comparative adverse events in AI and SERM users. That doesn't mean "choose the one with fewer posts complaining." It means accept tradeoffs like an adult.
What outcomes should you expect during and after PCT?
People want certainty here. The endocrine system does not care.
Libido and mood
If a SERM is working in the intended way, you might see libido return in fits and starts, sleep improve, morning erections become less random, and mood swings settle. Or you might feel emotionally sharp but oddly irritable. Clomiphene can do that.
AIs, when used at the wrong time, can produce the classic low-estrogen vibe: low sex drive, anxious flatness, brittle motivation, and that specific "my joints feel 10 years older" complaint. If you're the type who thinks estrogen is only a water balloon, you learn fast.
One under-discussed quirk: clomiphene has been associated with changes in IGF-1 in a substantial portion of male patients, which matters if you care about training recovery and overall metabolic signaling. The data is not internet myth: IGF-1 changes reported with clomiphene therapy.
Water retention and blood pressure
High E2 during or right after a cycle can drive water retention, higher blood pressure readings, and that puffy look some bodybuilder types pretend is "just sodium." Sometimes it is sodium. Sometimes it's cycle estrogen management being ignored until you feel like a balloon animal.
AIs can help this when high estrogen is real and measured. SERMs might help certain breast-tissue symptoms but won't reliably dry you out because they are not primarily lowering serum estrogen levels.
Gynecomastia risk
Gynecomastia is a tissue outcome, not just a lab outcome. Breast tissue cares about receptor signaling, local conversion, and duration of exposure.
Tamoxifen is a common tool because it can block estrogen receptors in breast tissue. If you're in an active flare (itching, tenderness, that "uh oh" nipple sensitivity), the receptor-level effect is the point. If you're trying to prevent it by obliterating estradiol with an inhibitor, you can end up trading one problem for another.
Use a phase-based decision framework

This is the part where people beg for a timetable. I'm not giving you that. I will give you a framework that makes it harder to do something dumb.
On-cycle control
On cycle, estrogen can climb because aromatase has more substrate. That's where an aromatase inhibitor belongs, if you need it, because you're managing production while exogenous androgens are driving the system. If you're cruising on testosterone replacement therapy, same logic: you're not "restarting," you're controlling conversion.
Also, the "estrogen rebound" fear gets exaggerated into superstition. Some rebound is real in the sense that when you stop suppressing aromatase, conversion resumes. The bigger issue is people oversuppress, then swing the other direction.
Transition window
The transition window is the awkward period where the long esters are clearing, hormones are shifting, and your brain is trying to read a dashboard where half the gauges are broken.
This is the zone where people panic-dose inhibitors because they feel soft, watery, moody, or anxious. Sometimes that's high estrogen. Sometimes it's withdrawal from supraphysiologic androgens plus cortisol and sleep debt and life.
If you're using hCG, this is also where timing matters, because hCG can preserve testicular function but it can be suppressive at the hypothalamus-pituitary level in practice. I like the staged logic described in this overview of hCG and SERMs in PCT, with the caveat that "support" is not "restart."
Post-cycle restart
This is where SERMs earn their reputation. You're trying to restore signaling and avoid prolonged endogenous testosterone inhibition. SERMs help the feedback loop wake up.
AIs here are rare and tactical, not foundational. If you have labs showing high estradiol with symptoms that actually match, an aromatase inhibitor post cycle can be a short bridge. If you are using it because you're scared of estrogen existing, you're probably sabotaging your own recovery.
Here's a compact comparison that keeps the jobs straight:
| Phase | Typical goal | Tool that usually fits | What "success" looks like |
|---|---|---|---|
| On-cycle | control excess estrogen symptoms | aromatase inhibitors (if needed) | fewer high-E2 symptoms, stable BP, stable mood |
| Transition | avoid swings, confirm with labs | minimal intervention unless clear issue | fewer drastic changes week to week |
| Post-cycle restart | restore LH/FSH and natural testosterone production | SERMs | LH/FSH rise, total testosterone and free testosterone improve, symptoms trend up |
Spot the wrong tool from symptoms and labs
Symptoms matter. Labs matter. The trap is treating either one like gospel.
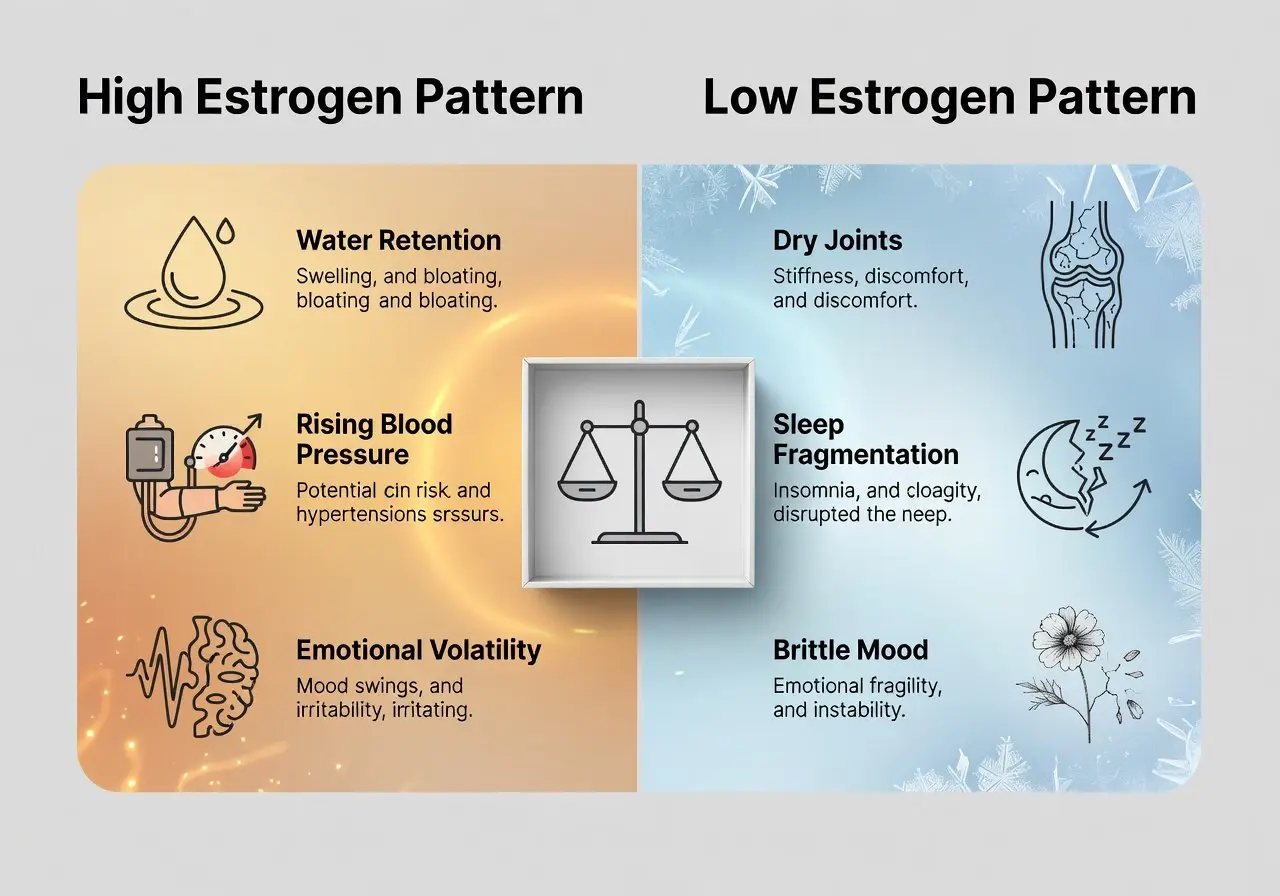
High-estrogen pattern
High estrogen tends to look like water retention, rising blood pressure, emotional volatility, libido that feels "crowded out," and sometimes worsening nipple sensitivity. Labs may show elevated estradiol, but context matters, including timing relative to last injections and AI use.
If your E2 is high and you're using only a SERM while expecting water weight to vanish, you're asking a screwdriver to do a wrench's job.
Low-estrogen pattern
Low estrogen is its own kind of misery: dry joints, low libido, erectile dysfunction, sleep fragmentation, irritability, and a sort of bleak, brittle mood. Labs may show estradiol that's pushed too low, often because an inhibitor was used aggressively or without measuring.
And the long-term angle is not cute. Aromatization matters for bone density and even physical function in men, which is part of why chronic suppression can be a bad plan: why aromatization supports bone health and gait speed.
False reassurance traps
Two traps show up constantly.
One is "my nipples stopped hurting so I'm fine," while LH/FSH and testosterone levels are still in the basement.
The other is "my testosterone bounced on paper so I'm recovered," while you're living with mood swings and low sex drive because estradiol got cratered or because you're reading the wrong assay.
The HAARLEM study discussion is a sobering reminder that real-world PCT outcomes aren't as magical as forums sell them, and that user behavior is messy: a critical look at PCT efficacy claims.
Test estradiol the right way
Estradiol testing is where a lot of "I swear my estrogen is high" stories go to die.
Sensitive assay choice
If you only remember one thing, remember this: ask for a sensitive estradiol assay (often LC/MS). A standard estradiol immunoassay can be inaccurate in men, especially at lower ranges. You want an estradiol assay that doesn't guess.
Call it a sensitive test, call it the "male" method, call it LC-MS/MS. Just don't call a blurry number "precision."
Timing and confounders
Timing is half the art. Test too soon after changing a SERM or inhibitor and you're chasing noise. Test while you're sleep-deprived, inflamed, drinking more alcohol, or coming off a hard cut and you'll also chase noise. Confounders are boring, which is why they ruin people.
- Recent AI changes can temporarily distort the number and how you feel.
- hCG use can raise intratesticular testosterone and aromatization, shifting estradiol.
- Big body composition shifts change aromatase activity because fat tissue is hormonally active.
Interpret E2 in context
Estradiol is not a standalone villain. Interpret it with total testosterone, free testosterone, LH/FSH, SHBG, symptoms, and your actual phase of cycle therapy. A "normal" estradiol number can still feel bad if testosterone is low; a "high-ish" number can be tolerable if androgen levels and blood pressure are stable.
If you want a clinical framing of aromatase inhibitor use specifically for elevated estradiol in men, not bodybuilding folklore, this review is a decent anchor: clinical perspective on AI therapy for high estradiol.
Avoid common safety mistakes and known risks
Most hormonal disasters come from the same small set of behaviors: treating estrogen like a toxin, changing too many variables at once, and using symptoms as the only compass.
SERMs carry their own baggage: visual disturbances can happen, mood changes can happen, and you're messing with estrogen receptors across tissues. AIs can mess with lipids, joints, libido, and potentially bone over time. Both can create serious side effects when misused, especially stacked carelessly.
One thing I wish people would stop doing is "chasing dryness." Low estrogen is not a trophy. If your joints hurt, sleep is wrecked, sex drive is gone, and you feel vaguely depressed, that is not you being "dialed."
And since it comes up constantly: yes, some people combine a SERM with an AI for a narrower goal of improving the testosterone/estradiol ratio, and there is research showing ratio changes when anastrozole is added to tamoxifen in certain contexts. That is not permission to freestyle. It's a reminder that the endocrine system responds to levers, and the levers have labels for a reason: data on combined tamoxifen and anastrozole effects on the T/E2 ratio.
Follow-up questions to pressure-test your plan
If you can answer these without hand-waving, you're already ahead of most of the internet.
- What phase are you in right now: on-cycle, transition, or post-cycle restart?
- Are you choosing a tool based on symptoms alone, or symptoms plus labs from the same week?
- If you feel bad, do your complaints match a high estrogen pattern or a low estrogen pattern?
- If hCG is in the mix, do you understand what it's supporting versus what it might suppress upstream?
FAQ
Can I do PCT with an AI instead of a SERM?
Sometimes testosterone rises with aromatase inhibition, but for most PCT goals, SERMs are the more direct tool for restoring LH/FSH signaling. Using an inhibitor as the backbone is a common way to feel worse and recover slower.
Do SERMs lower estradiol?
Not reliably. They primarily change estrogen receptor signaling. Serum estradiol can stay the same or even rise.
Is "estrogen rebound" the big enemy?
The bigger enemy is oversuppression and yo-yo decision-making. Stop treating estrogen like a jump scare and start treating it like a variable you measure.
What estradiol number is "too high"?
There isn't a universal cutoff that applies to every man in every phase. Use the sensitive assay, look at symptoms, and interpret alongside testosterone, LH/FSH, and blood pressure.
Conclusion
If you take nothing else: SERMs are usually the restart lever, aromatase inhibitors are the production-control lever. PCT is supposed to get your hormonal signaling back online, not just smooth out your mood for a weekend.
The people who do best treat recovery like a staged transition, not a panic response. Measure estradiol with the right assay, respect what estrogen does for men, and stop swapping tools mid-flight because one day felt weird. That's how "PCT" turns into a long, expensive, avoidable slog.
Articles

Steroids work. Yes, you certainly have to battle negative side effects that will almost appear in concert and in ratio with the positive effects, but they certainly do work.

All anabolic steroids are oil-or water-based intended for intramuscular injection. This means that the needle must pass through the skin, subcutaneous tissue and enter into the muscle. Parts of the body, which usually inject are: buttocks, lateral thigh and the deltoid muscle arms.

Sermorelin is a growth hormone-releasing hormone (GHRH) peptide that stimulates the body’s natural GH production instead of supplying synthetic HGH directly. This guide explains Sermorelin benefits, dosage protocols, recovery effects, sleep support, side effects, and safety considerations.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.