


Why Aromatase Inhibitors During PCT Crash Estrogen and Hurt Recovery
Most of us have been there: you've just wrapped a steroid cycle, you're mentally ready to transition into recovery, and somewhere in the noise of forum posts and Reddit threads, someone insists you should keep running your aromatase inhibitor straight through PCT. Sounds logical on the surface. Control estrogen, protect against gyno, stay "dry." Except that advice is, in a lot of real-world scenarios, quietly sabotaging the exact recovery you're trying to achieve.
The short answer is this: aromatase inhibitors should be tapered off before PCT begins, not carried through it, because suppressing estrogen to rock-bottom levels during recovery actively stalls the hypothalamic-pituitary-testicular axis (HPTA) restart your body desperately needs. SERMs like tamoxifen, clomid, or enclomiphene are the preferred tools for PCT because they block estrogen at the receptor level in the pituitary without nuking circulating estradiol. That distinction matters more than most people realize.
Let me walk through why, and more importantly, how to handle the transition so you're not white-knuckling through crashed E2 symptoms while your endocrine system tries to find its footing again.
Why Aromatase Inhibitors Hurt Recovery During PCT

Estrogen's Role in the HPTA Restart
There's a pervasive myth in bodybuilding circles that estrogen is the enemy. Full stop. And on cycle, sure, managing aromatization makes sense because supraphysiological testosterone doses can flood the system with estradiol, leading to water retention, gyno, mood swings, the whole catalog of unwanted side effects.
But estrogen is not a villain during recovery. It's a signaling molecule. Your hypothalamus uses circulating estradiol as one of its primary feedback cues to gauge whether the body needs more gonadotropin-releasing hormone (GnRH). If estrogen levels are adequate (not high, not crashed), the hypothalamus reads the environment as "time to ramp up production." Wipe out estrogen entirely, and that feedback loop gets garbled. A comprehensive review of aromatase inhibitors in men confirms that complete estrogen deficiency is genuinely detrimental to male health across multiple systems, including bone metabolism, sexual function, and cardiovascular markers.
So when someone runs a full-dose AI through PCT, they're essentially cutting one of the wires the HPTA needs to reboot cleanly.
How Crashed E2 Stalls Testosterone Production
Think about it mechanistically. SERMs work by occupying estrogen receptors at the pituitary, which tricks the gland into thinking estrogen is low at that specific tissue. The pituitary responds by increasing LH and FSH output, which tells the testes to start producing testosterone again. That's the whole game plan.
Now layer an AI on top of that. You're not just blocking the receptor; you're eliminating the substrate entirely. Circulating estradiol drops into single digits. The pituitary is already being told "estrogen is low" by the SERM, and now the actual systemic estrogen is low because the aromatase enzyme has been crushed. You've doubled down on a signal that didn't need doubling. Clinical evidence shows PCT users had significantly higher serum testosterone following AAS cessation compared to those who skipped recovery drugs entirely, but that benefit hinges on running the right drugs, not stacking every anti-estrogen tool you own.
Low estradiol doesn't just feel bad. It actively impairs the recovery process by reducing the quality of the hormonal signal chain you need functioning at full capacity.
Signs of Estrogen Over-Suppression
And yeah, the symptoms of crashed estrogen are miserable. They overlap annoyingly with low testosterone symptoms, which is part of why people misread them:
- Joint aches and stiffness that feel disproportionate to your training load
- Dry, cracking skin, especially lips and knuckles
- Erectile dysfunction or severely blunted libido even when testosterone is technically recovering
- Flat, almost dissociative mood, not quite depression but a persistent emotional numbness
- Fatigue that sleep doesn't fix
Research into anastrozole dose escalation demonstrates just how dose-dependent estrogen suppression is, and how quickly things can tip from "managed" to "obliterated" with only modest increases.
If you're weeks into PCT and experiencing that cluster, the AI is almost certainly the culprit, not insufficient estrogen blockade.
SERMs vs AIs: What Actually Belongs in PCT
How SERMs Stimulate Natural Testosterone
SERMs, selective estrogen receptor modulators, are the backbone of any serious post-cycle therapy protocol for a reason. Tamoxifen (Nolvadex) and clomiphene (Clomid) occupy estrogen receptors in the hypothalamus and pituitary, tricking those tissues into upregulating GnRH and gonadotropin output. The rest of the body still "sees" circulating estradiol, which means bones, joints, cardiovascular tissue, and the brain all retain the estrogen signaling they need.
That selective mechanism is the whole point. You get the LH/FSH stimulation without the collateral damage of systemically destroying estrogen.
Why AIs Work Against That Goal
Aromatase inhibitors do something fundamentally different. They reduce estrogen production at the enzyme level, either reversibly (anastrozole, letrozole) or irreversibly (exemestane, a steroidal AI). On cycle, this is useful because you're swimming in exogenous testosterone that aromatizes aggressively, especially if you carry higher body fat. Data comparing letrozole and exemestane shows both can suppress serum estrone and estradiol substantially, which is exactly what you want when managing high estradiol during a blast.
During PCT, though, your testosterone production is a trickle. There's barely any substrate for the aromatase enzyme to convert. Suppressing what little estrogen your body is producing at that stage is counterproductive. You're fighting the recovery instead of supporting it.
Nolvadex, Clomid, and Enclomiphene Compared
| SERM | Typical PCT Dose | Duration | Notes |
|---|---|---|---|
| Tamoxifen (Nolvadex) | 20 mg/day | 4–6 weeks | Well-studied, reliable LH stimulation, some visual side effects rare |
| Clomiphene (Clomid) | 25–50 mg/day | 4–6 weeks | Stimulates both LH and FSH robustly; mood changes reported more often |
| Enclomiphene | 12.5–25 mg/day | 4–8 weeks | The trans-isomer of clomid, fewer estrogenic side effects, gaining popularity |
Enclomiphene deserves a separate mention because its before-and-after timelines tend to show a more gradual, steady climb rather than an aggressive spike and crash pattern. People either expect magic fast or assume it's useless because they're impatient. The more realistic view is that response builds over weeks, with many reporting the most noticeable improvements several months in.
How to Dose AIs on Cycle Without Overcorrecting

Standard Anastrozole and Exemestane Protocols
On cycle, AI dosing should be the minimum effective amount to keep estrogen-related side effects at bay without driving E2 into the ground. The mistake I see constantly is people running a fixed schedule regardless of symptoms or bloodwork.
Common starting points for a moderate testosterone cycle (400–500 mg/week):
- Anastrozole (Arimidex): 0.25–0.5 mg every other day, adjusted based on labs
- Exemestane (Aromasin): 12.5 mg every other day or every third day
- Letrozole: generally reserved for emergency gyno flare-ups at 0.5–1.25 mg; too potent for routine use
The pharmacokinetics of third-generation AIs show that even anastrozole, with its roughly 42-hour half-life, accumulates meaningfully over a few weeks. What feels like a low dose on day one becomes a much heavier suppressive load by week four.
Labs and Symptoms Over Fixed Schedules
I'll take a stance here: chasing a specific estradiol number on a lab printout is where most guys go wrong. The relationship between TRT and estrogen is not a spreadsheet variable you can micromanage into perfection. Rising E2 on cycle is expected because there's more substrate for conversion. Your north star should be the trend across labs combined with actual symptoms, not a panic response to a single high reading.
If you're not holding excessive water, you don't have tender breast tissue, your mood is stable, and your sexual function is fine, you probably don't need to bump the AI dose just because estradiol came back at 55 pg/mL instead of 30.
Common Dosing Mistakes That Create Problems Later
The most frequent error is preemptive dosing. Running an AI from day one of a cycle "just in case" before any estrogen issues have actually manifested. This front-loads suppression and makes it nearly impossible to gauge your actual aromatization rate. The second mistake is refusing to adjust downward. People find a dose that controls a symptom and then cement it as gospel for every cycle, every compound, regardless of how their body fat, lean mass, or total dose has changed.
Bone mineral density concerns from prolonged estrogen suppression aren't just theoretical. Even healthy men running AIs chronically face measurable impacts, and cardiovascular and lipid profile data from larger trials paints a similar cautionary picture.
Taper Your AI Before PCT Starts
When to Begin Reducing the Dose
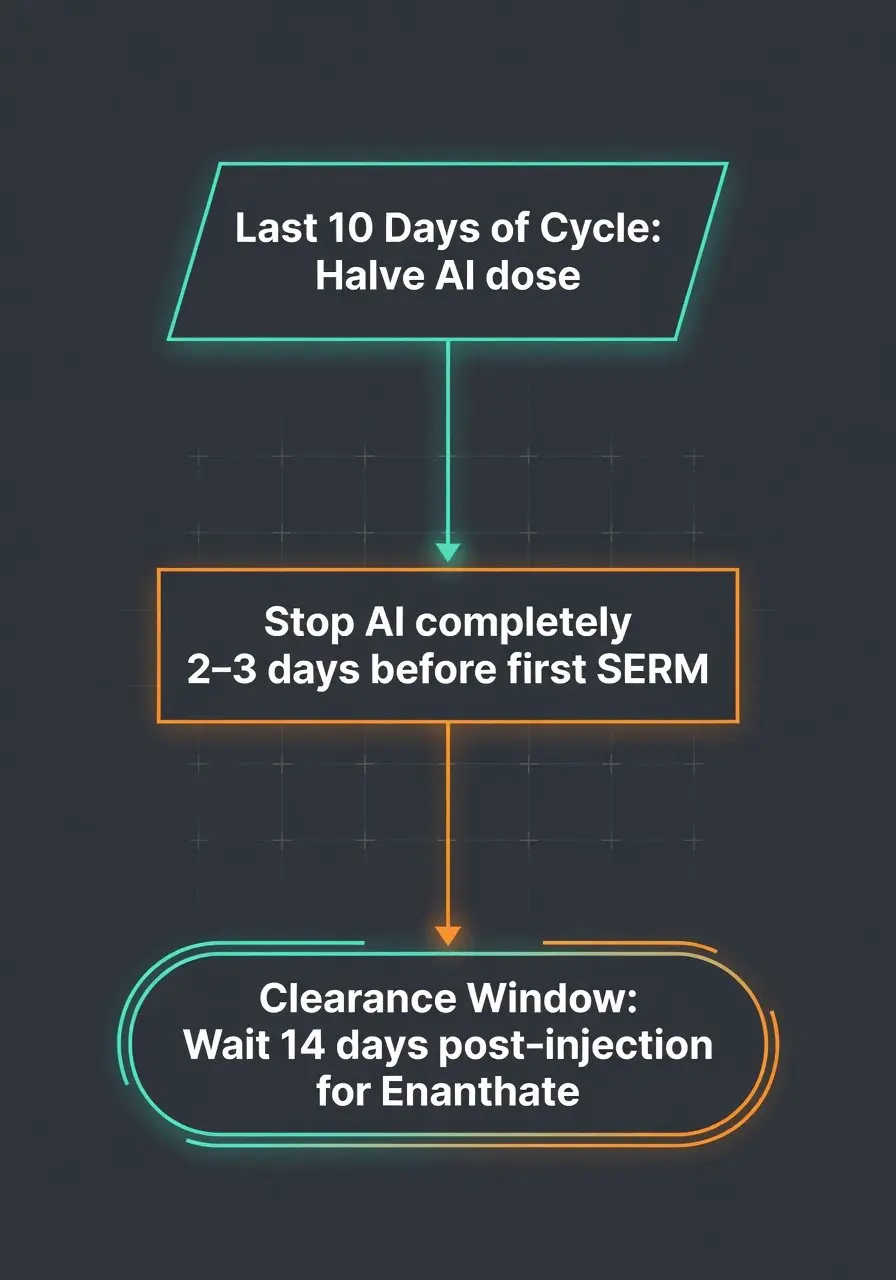
This is the part nobody talks about with enough specificity. You should begin tapering your AI in the final week or two of your cycle, not abruptly stopping it the day PCT begins. A sudden cessation of anastrozole, for instance, can trigger an estrogen rebound because the aromatase enzyme recovers faster than most people expect. You go from suppressed to flooded, and now you're starting PCT with wildly unstable hormone levels.
A practical approach: halve your AI dose during the last 10 days of your cycle. If you were running 0.5 mg anastrozole EOD, drop to 0.25 mg EOD, then stop entirely 2–3 days before your first SERM dose.
Transition Timeline Based on Ester Half-Life
The gap between your last pin and your first PCT dose depends entirely on the ester attached to whatever anabolic compound you were running. Testosterone enanthate has a half-life around 4.5 days, so PCT typically starts 14 days after the last injection. Testosterone propionate clears much faster, maybe 3 days to start PCT. Longer esters like undecanoate can mean waiting three weeks or more.
Your AI taper should align with this clearance window. As the exogenous testosterone drops, so does aromatization. By the time you start your SERM, the AI should already be out of your system. Clinical evidence on spontaneous versus facilitated recovery confirms that while the body can eventually normalize without intervention, PCT accelerates the process considerably, but only when the hormonal environment isn't being actively sabotaged by concurrent AI use.
What a Practical SERM-Based PCT Protocol Looks Like
PCT isn't a one-size recipe, even when the structure looks similar. The timing should be based on what you used and how long it lingers. Starting too early means you're basically fighting while the drug is still actively suppressing feedback signals. Starting too late means you've already slid into the worst suppression window, and mood, libido, strength, everything takes a nosedive.
A standard protocol after a 12-week testosterone enanthate cycle might look like: wait 14 days post-last injection, then run tamoxifen at 20 mg/day for 6 weeks. Or enclomiphene at 12.5–25 mg/day for 6–8 weeks if you prefer the milder side effect profile. No AI during this window. Period.
If you're genuinely concerned about estrogen rebound in the first few days, a single low dose of exemestane (12.5 mg) as a bridge is about as aggressive as it should get. Exemestane being a steroidal AI means its mechanism of irreversible inhibition provides a more predictable suppression window without the boomerang effect that non-steroidal options like anastrozole can produce.
One more thing worth mentioning: a study on self-administered PCT drugs found that over 34% did not contain the declared active ingredients. Source quality matters. If your SERM is bunk, your entire recovery plan collapses regardless of how perfect your protocol looks on paper.
How Do You Know Estrogen Is Too Low During Recovery
Bloodwork. That's the definitive answer. But practically speaking, most people won't run labs every week during PCT, so symptom awareness becomes your early warning system. The joint dryness is usually the first thing. Then the libido drop that feels qualitatively different from low-T libido, more like complete absence of interest rather than difficulty performing. Mood becomes eerily flat.
If you're experiencing these and you're running an AI during PCT, stop the AI immediately. The SERM alone should be managing estrogen activity at the pituitary. You do not need systemic estrogen suppression during this phase.
Get a sensitive estradiol assay (the LC/MS method, not the standard immunoassay) around week 3–4 of PCT. If E2 is below 15 pg/mL, something is wrong, and the AI is the most likely offender.
Why Month Three Is the Real Checkpoint for HPTA Recovery
Most people evaluate their PCT success way too early. Week two of SERM use, they feel off, panic, and start tweaking things. But HPTA recovery doesn't operate on a two-week timeline.
The real signal, the one that tells you whether your axis is genuinely recovering, usually appears around month three. That's when enclomiphene results typically stabilize and when post-SERM labs can give you a meaningful snapshot of where your endogenous production has landed. It's like switching training blocks: early on you get random fluctuations in water, sleep, motivation. The real signal is when your baseline performance and day-to-day recovery start behaving like they've found a new normal.
Pull comprehensive labs at the 10–12 week mark post-cycle start (or 4–6 weeks after finishing your SERM). Total testosterone, free testosterone, LH, FSH, sensitive estradiol, and SHBG. That panel tells you whether the restart actually took or whether you need further intervention.
FAQ
Can I run a low-dose AI during PCT "just for safety"? Strongly not recommended. Even a reduced dose of anastrozole or letrozole during PCT can push estradiol low enough to impair HPTA signaling. SERMs handle the estrogen modulation you need at the tissue level without reducing systemic E2. The StatPearls clinical overview of aromatase inhibitors reinforces that these drugs are potent even at therapeutic doses and should be used with careful monitoring.
What if I get gyno symptoms during PCT? Tamoxifen is actually your first-line defense here because it directly blocks estrogen receptors in breast tissue. That's literally what it was designed for. A brief bump to 40 mg/day for a week, then back to 20 mg, handles most flare-ups without touching your circulating estradiol.
How long does it take for estrogen to normalize after stopping an AI? With anastrozole, estrogen levels typically begin recovering within 3–5 days of the last dose. Exemestane, because it permanently deactivates the aromatase enzyme molecules it binds to, requires new enzyme synthesis, which can take 7–14 days for meaningful recovery. Plan your taper accordingly.
Conclusion
PCT is damage control, not a victory lap. The whole point is restarting a suppressed endocrine system as efficiently as possible, and aromatase inhibitors actively work against that goal when used during recovery. Taper your AI before PCT begins, let your SERM do its job at the pituitary, and resist the urge to micromanage estrogen into the floor. Your body needs that estradiol to read the room and start producing testosterone again.
Run labs. Track symptoms over trends, not single data points. Give the process time, because month three is usually where you finally know what's real. And above all, stop treating PCT like a fixed recipe. What you took, how long you ran it, your body fat, your aromatization rate: these variables matter, and no forum protocol can account for all of them. The guides help, but they don't replace follow-through, bloodwork, and not ignoring what your body is telling you.
Articles

GH stands for growth hormone, a hormone produced by the pituitary gland that plays a key role in growth, recovery, metabolism, and hormone regulation. This guide explains GH medical terminology, HGH therapy terms, and the most important growth hormone definitions used in medicine and bodybuilding.

Discover the best peptides for sleep, recovery, and growth hormone support. Learn how Ipamorelin, CJC-1295, GHRP-6, and other GH peptides improve deep sleep and recovery.

BPC-157, TB-500, and CJC-1295 are popular recovery peptides used for tissue repair, healing support, and growth hormone optimization. This guide explains how these peptides work, compares their evidence and mechanisms, and explores potential benefits, risks, and safety considerations.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.