


Subcutaneous Injection vs Oral Capsule Peptide Delivery for Joint Inflammation

Most people start looking into peptide therapy for joint inflammation after they've already tried the usual rotation of NSAIDs, physical therapy, maybe a cortisone shot that wore off too fast. By the time you're Googling "subcutaneous injection vs oral capsules for peptide delivery," you're not a beginner. You're someone who wants to know which route actually gets the compound where it needs to go, and how quickly you can expect relief.
So let me give you the short version upfront: subcutaneous injection delivers peptides into systemic circulation with bioavailability typically between 50% and 80%, producing noticeable anti-inflammatory effects within days to a couple of weeks. Oral capsules, by contrast, fight through enzymatic degradation and pH shifts in the gut, arriving at a baseline oral bioavailability of roughly 1% to 2% for most unmodified peptide formulations, which means onset of meaningful relief stretches into weeks or months. The delivery route you choose isn't a minor detail. It fundamentally changes the pharmacokinetic profile, the therapeutic timeline, and honestly, whether you're getting your money's worth.
Now, the longer version. Because this topic has more layers than most people realize.
How Bioavailability Differs Between Injection and Oral Peptides
Subcutaneous Absorption Pathways
When you inject a peptide like BPC-157 subcutaneously, you're depositing it into the fatty tissue layer just beneath the skin. From there, the compound diffuses into capillaries and the lymphatic system, eventually reaching the bloodstream. The absorption mechanisms through this fatty tissue layer follow what researchers call a dual-pathway model, a combination of direct vascular uptake and slower lymphatic transport. What this means practically: peak plasma concentration (Tmax) arrives relatively fast, often within 30 minutes to a few hours depending on injection site and molecular weight.
Injectable BPC-157, for instance, bypasses the gastrointestinal tract entirely. No gastric juice to contend with, no enzyme peptidase activity chopping the molecule apart before it ever reaches circulation. That's why subcutaneous bioavailability figures land so much higher compared to oral delivery. The peptide arrives largely intact.
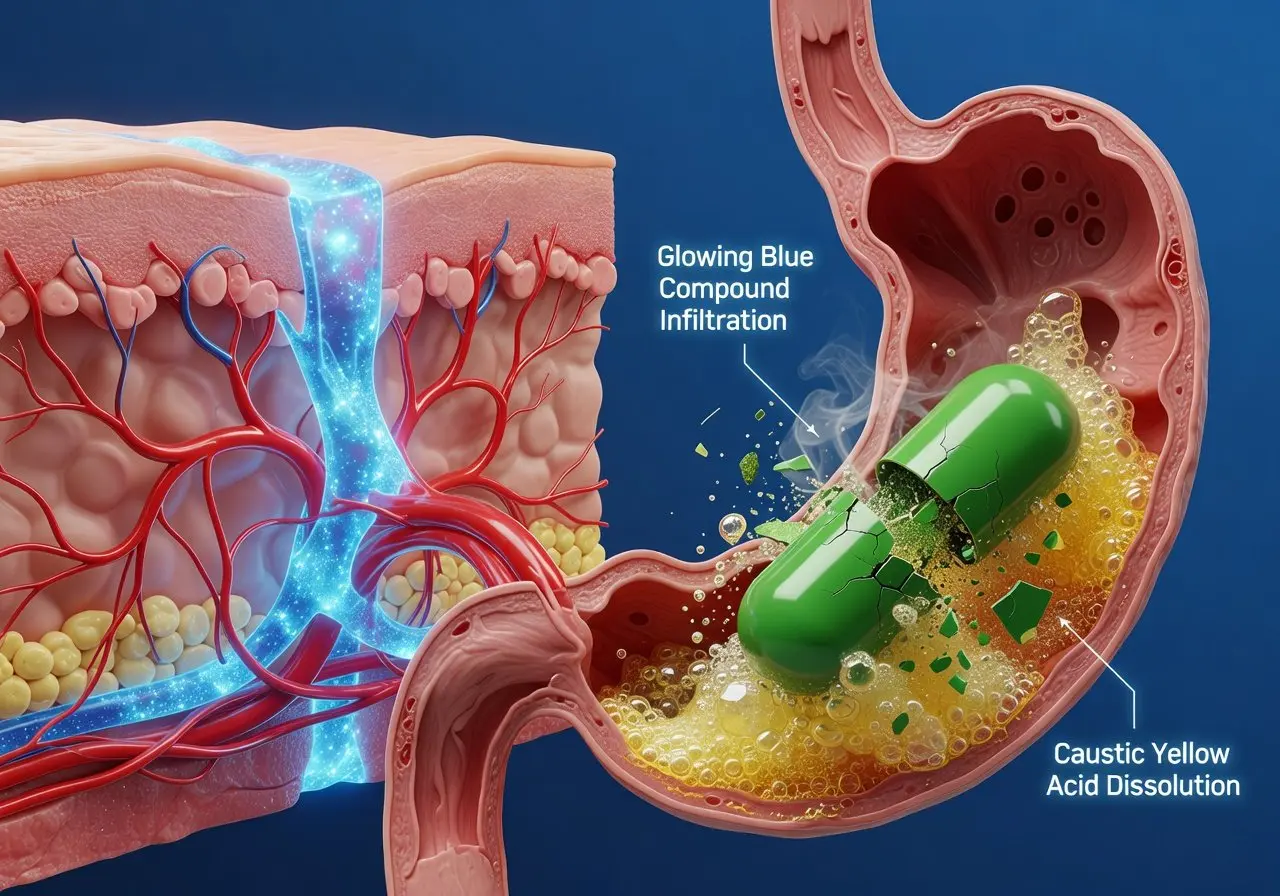
Oral Capsule Degradation Barriers
Oral BPC-157 capsules face a genuinely hostile environment. The moment a capsule dissolves in your stomach, the peptide encounters hydrochloric acid, pepsin, and a pH that can drop below 2. Whatever survives the stomach then moves into the small intestine, where pancreatic proteases and the intestinal epithelial barrier present another gauntlet. The epithelial tight junctions of the gut wall are designed to keep large molecules out of the bloodstream. Peptides, being chains of amino acids, are exactly the type of molecule this barrier evolved to break down and exclude.
Some advanced drug delivery approaches try to solve this. Permeation enhancers, enteric coatings, even liposome encapsulation can improve oral bioavailability marginally. Oral semaglutide, one of the few FDA-approved oral peptide drugs, uses a specific permeation enhancer called SNAC to achieve clinically relevant absorption, but even then the dosing has to be dramatically increased compared to its injectable counterpart. We're talking about needing sometimes 100-fold more compound orally to match what a small subcutaneous injection achieves.
Side-by-Side Bioavailability Comparison
|
Factor |
Subcutaneous Injection |
Oral Capsule |
|---|---|---|
|
Typical bioavailability |
50%–80% |
1%–2% (unmodified); up to ~10% with enhancers |
|
Time to peak plasma level |
30 minutes–4 hours |
1–3 hours (if absorbed at all) |
|
Enzymatic degradation risk |
Minimal |
High (stomach acid, pepsin, intestinal proteases) |
|
Dosing efficiency |
Low dose needed |
Substantially higher dose required |
|
Systemic exposure consistency |
Predictable |
Highly variable based on fed/fasted state, gut health |
That table should make the pharmacokinetic gap obvious. When someone tells you BPC 157 capsules work "just as well" as injections, the numbers simply don't support that claim without significant formulation engineering.
Why Delivery Route Changes How Peptides Reach Inflamed Joints
Local Tissue Targeting via Injection
There's a widespread belief in peptide therapy circles that injecting near the site of inflammation, say, close to an inflamed knee or shoulder, creates a localized therapeutic effect. This is partially true but also somewhat misleading. Subcutaneous injection deposits the peptide into tissue, yes, and there is a local concentration gradient before systemic distribution occurs. But the compound doesn't stay put. Peptide clearance and redistribution data show rapid movement into systemic circulation regardless of injection site.
That said, the initial local concentration does matter for tissues with poor blood supply, like tendons, cartilage, and the synovium surrounding joints. Getting even a transient high concentration near the inflamed tissue could theoretically influence local repair signaling before the peptide dilutes systemically.
Gut-First Processing via Oral Route
Oral peptides that manage to survive digestion face first-pass metabolism in the liver before reaching general circulation. This gut-first processing further reduces the amount of active peptide available for distant tissue targets like an inflamed joint. The physicochemical barriers in the gastrointestinal tract mean that by the time any BPC-157 from a capsule reaches your knee, you're working with a fraction of a fraction of the original dose.
Interestingly, oral BPC-157 may offer something injections don't: direct interaction with the gut lining, which has implications for gastrointestinal repair and neuroprotection pathways that BPC-157 is associated with in preclinical research. So the oral route isn't useless. It's just aimed at a different target, one that might not be your primary treatment goal if joint inflammation is what you're trying to address.
Systemic vs. Localized Therapeutic Effects
The practical distinction here is straightforward. Injectable BPC-157 and similar peptide therapies create systemic exposure that reaches inflamed joints with more intact compound. Oral BPC capsules, even quality formulations with enteric coating, deliver their strongest effects along the GI tract, with limited systemic delivery for downstream joint targeting. If inflammation control at a specific joint is the goal, the injection route has a pharmacological advantage that's hard to argue with.
What Joint Inflammation Relief Timelines Look Like for Each Method
Onset of Action After Injection
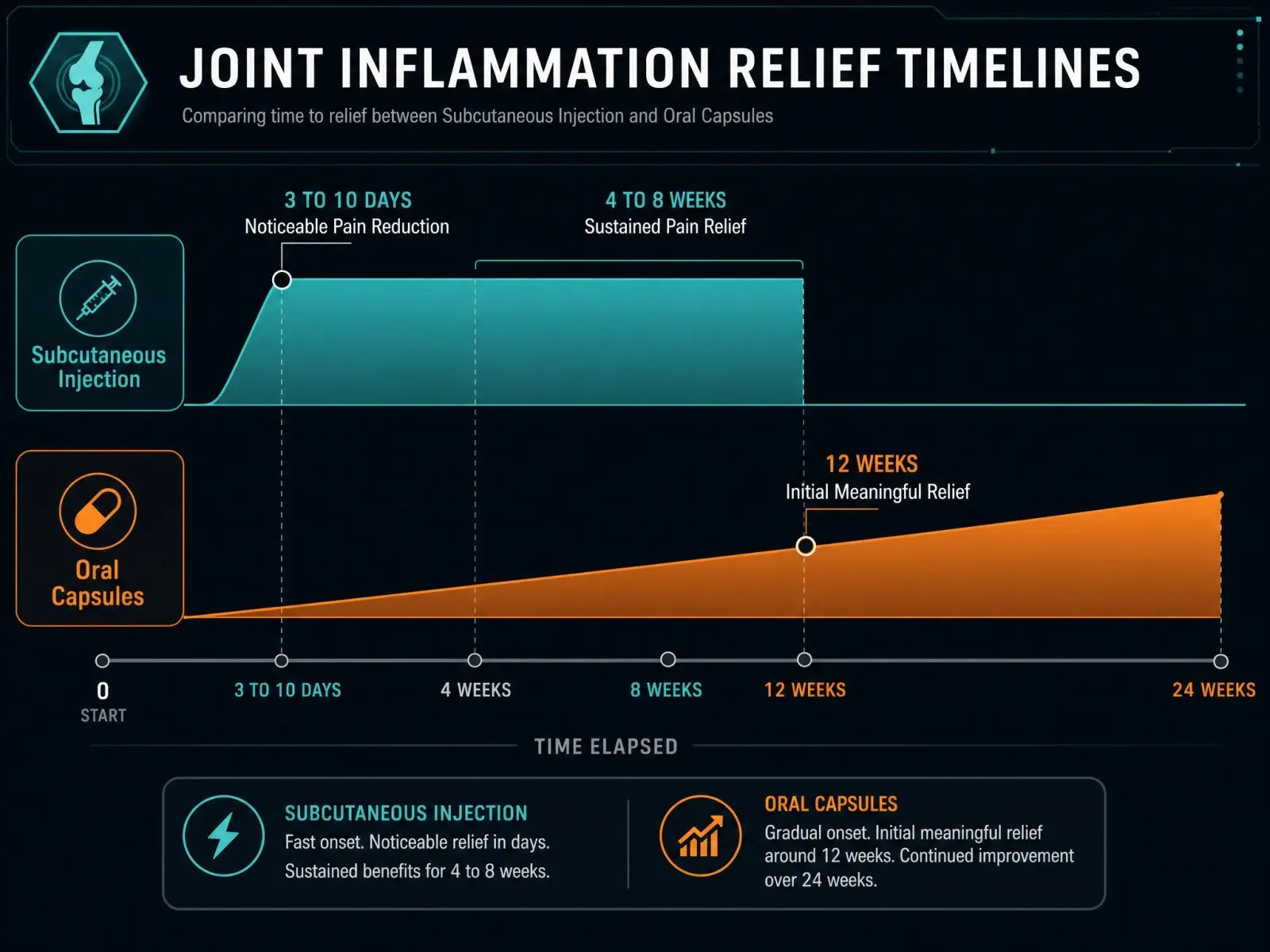
Anecdotal reports from patients using injectable BPC-157 for soft tissue injuries describe noticeable pain reduction within 3 to 10 days. Some climbers and athletes have documented their experience recovering from pulley and tendon injuries with a similar arc: significant symptom relief within the first week or two, with continued improvement over 4 to 8 weeks of a typical peptide protocol.
But I want to be honest about something. That timeline is exactly the window where a lot of other things also happen. You stop the aggravating activity. You calm local irritation. Your mechanics improve because you can't do the thing that kept hurting you anyway. So any supplement, or even a placebo, can get credit during that window. I've come to think of these rapid-relief stories as compelling but not conclusive.
Onset of Action After Oral Capsules
Oral peptide therapies for joint inflammation generally operate on a longer timeline. Clinical trials investigating bioactive collagen peptides for joint pain typically assess outcomes at 12-week intervals, and that seems about right for what oral delivery can realistically achieve. When you factor in the low oral bioavailability and the variable absorption driven by individual gut health, expecting meaningful joint-level effects from oral BPC 157 capsules in under a month feels optimistic.
Some multicenter clinical trials assessing oral peptide responses in rheumatoid arthritis have used 24-week endpoints, which gives you a sense of how seriously researchers take the extended timelines for oral formulations in inflammatory conditions.
Duration of Therapeutic Effects
Duration is trickier to pin down. Subcutaneous injection tends to produce therapeutic effects that last roughly as long as the dosing continues, with some carryover after cessation, potentially weeks, depending on the injury type and severity. Oral capsule formulations, when they work, tend to build effects cumulatively over months rather than producing acute spikes.
Think of it like this: injections are more like a concentrated dose of espresso, hitting fast and wearing off without continued administration. Oral capsules, when they contribute at all, behave more like a slow drip, gentle accumulation that requires adherence and patience.
Why "Feeling Better Fast" Does Not Equal Structural Recovery
This is where I get blunt. "I feel 90% better" is not the same as "the tendon or cartilage is biomechanically ready." In sports medicine and regenerative medicine alike, patients frequently mistake pain reduction for tissue restoration. You can feel functional long before you've regained full tissue tolerance, which is exactly how re-injury happens.
The community discussions around BPC-157 reveal this pattern clearly. The loudest voices aren't saying "this is scientifically established treatment." They're saying "it's the only thing I tried that matched the feeling of healing I expected." That's emotionally compelling but functionally dangerous if it leads you back to full loading too early.
Here's what matters more than how quickly your pain drops:
-
Whether imaging confirms structural improvement at the joint or tendon level
-
Whether progressive loading tests (not just pain-free daily activity) indicate restored capacity
-
Whether your medical provider agrees that the tissue has recovered sufficiently for return to activity
-
Whether you've addressed the mechanical or biomechanical factors that caused the inflammation in the first place
Body protection compound 157 might nudge healing. It might reduce inflammation signaling. But treating any peptide therapy as a standalone fix, without the "boring stuff" like rehab, gradual loading, and medical supervision, is a recipe for cycling through injuries indefinitely.
How to Match Delivery Method to Your Recovery Goals
Severity and Location of Inflammation
Acute, localized joint inflammation, a flared-up knee, an irritated rotator cuff, a pulley injury in the hand, these scenarios favor subcutaneous injection if you're going the peptide route at all. The reasoning is simple: you want maximum systemic exposure reaching the target tissue, and you want it relatively fast. For systemic inflammation or conditions involving gut-joint axis dysfunction (which is more relevant than people realize), oral peptides could play a supporting role, particularly given BPC-157's documented effects on gastric parietal cells and gut mucosal integrity.
Lifestyle and Compliance Factors
Let's be real. Not everyone is comfortable with injections. The needle, the reconstitution, the sterility protocols, it's a lot. Oral BPC 157 capsules are vastly more convenient, and adherence matters enormously for any therapy to produce results. If injection anxiety means you'll do it inconsistently, or skip it altogether after week two, the capsule form might deliver more total benefit simply because you'll actually take it.
When Injection Is Worth the Trade-Offs
Injection is worth the trade-offs when:
You're dealing with a diagnosed soft-tissue injury that's limiting function. You've already committed to a structured rehab program and want an adjunctive therapy. You have access to a clinic or medical provider who can guide dosage, injection technique, and monitoring. And critically, you're sourcing from a supplier that provides third-party certificates of analysis.
A TB 500 combination peptide protocol alongside BPC-157 is something you'll see discussed in sports recovery circles, and while the preclinical rationale is interesting, the clinical data in humans remains thin. This brings us to a point that can't be overstated.
Safety Risks, Sourcing Problems, and the Case for Medical Oversight
The biggest practical risk with peptide therapies, whether injectable or capsule formulations, isn't the compound itself. It's the sourcing. BPC-157 is not an FDA-approved prescription drug. It's sold as a research peptide, and the quality control varies wildly between suppliers. Contamination, underdosing, mislabeling, these are documented problems in the peptide products space.
My bias is simple: if a compound's effectiveness depends on whether you bought "the good one," then it's not reliable enough to call genuinely effective at scale. The "works for me" crowd is too often really saying "works for me with my specific supplier," and that's not reproducible medicine.
Medical supervision matters here for several reasons beyond just safety. A provider with your health history can assess whether peptide therapy makes sense given your medications, your diagnosis, and your treatment goal. They can monitor for adverse effects. They can also tell you when what you actually need is an MRI, a prescription drug, or surgery, not another vial of research compound.
Clinical guidance keeps you from falling into the trap of self-experimenting indefinitely without ever getting a proper diagnosis. And frankly, the current state of BPC-157 human trials doesn't yet support the level of confidence that online forums project.
Can You Combine Both Delivery Routes for Joint Inflammation?
Some patients and clinics do combine injectable and oral BPC-157, using subcutaneous injection for targeted systemic exposure while adding oral capsules for GI support or broader anti-inflammatory coverage. This isn't irrational from a mechanistic standpoint. The peptide-based targeted delivery strategies being researched suggest that multi-route approaches could theoretically address different tissue compartments simultaneously.
But "theoretically" is doing heavy lifting in that sentence. Without established dosage protocols for combined routes, you're essentially designing your own experiment. Provider guidance is non-negotiable here.
Does Peptide Source Quality Affect Outcomes More Than Route?
Honestly? I suspect it does, at least in the current market. Two people can follow the exact same injectable BPC-157 protocol, and if one has a quality formulation and the other got an underdosed or contaminated batch, their outcomes will diverge dramatically. This variable alone makes it nearly impossible to draw clean conclusions from user experience threads and community reviews.
Until peptide therapies for joint inflammation move through proper clinical trials with standardized formulations, sourcing will remain the wild card that muddies every conversation about efficacy.
FAQ
How long does it take for BPC-157 injections to reduce joint inflammation? Most anecdotal reports describe noticeable pain reduction within 3 to 14 days with subcutaneous injection, though structural recovery takes significantly longer.
Are oral BPC-157 capsules effective for joint inflammation? Oral BPC capsules have substantially lower bioavailability than injections. While they may offer some digestive support and gradual anti-inflammatory effects, meaningful joint-level relief typically requires 8 to 12 weeks or more with oral peptide formulations.
Is BPC-157 FDA-approved for joint inflammation treatment? No. BPC-157 is not an FDA-approved medication for any medical use. It's classified as a research compound and should only be used under clinical guidance with proper medical supervision.
Can I switch from oral capsules to subcutaneous injections mid-treatment? You can, but dosage adjustments are necessary given the vast difference in bioavailability between routes. Consult your medical provider before changing your peptide protocol.
Conclusion
Choosing between subcutaneous injection and oral capsules for peptide delivery in joint inflammation isn't really a debate about convenience vs. inconvenience. It's a question of pharmacokinetics, and the figures aren't subtle. Injections deliver more intact peptide, faster, with more predictable systemic exposure. Oral capsules are easier to take but face brutal degradation barriers that most candidate peptide molecules simply can't overcome without sophisticated formulation technology.
My non-neutral bottom line: I think BPC-157 peptides are overhyped as a certainty but plausible as a "might help, might nudge healing" adjunct for certain soft-tissue problems, especially when combined with structured rehab and proper medical oversight. Treat anecdotal recovery stories as hypothesis generation, not as controlled evidence. Choose your delivery route based on your specific treatment goal, your injury severity, and your willingness to engage with the messy realities of sourcing and medical supervision. The peptide isn't the main event. The boring stuff, rest, rehab, gradual loading, that's still doing most of the work.
Articles

GH stands for growth hormone, a hormone produced by the pituitary gland that plays a key role in growth, recovery, metabolism, and hormone regulation. This guide explains GH medical terminology, HGH therapy terms, and the most important growth hormone definitions used in medicine and bodybuilding.

Trying to decide between Testosterone Enanthate vs Cypionate for TRT? Discover the real differences, half-life comparison, side effects, dosing tips, and which option is best for stable hormone levels.

Nutrition in bodybuilding is a type of diet aimed at changing the condition of the body. As a rule, such a diet is focused on increasing muscle mass.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.