


GH Medical Meaning Guide: Growth Hormone & Therapy Terms

Introduction
In a medical chart, GH almost always stands for growth hormone. If you're reading labs, a referral note, or a pharmacy prior auth, "GH" is shorthand for a real endocrine axis (pituitary to liver to tissues) that affects height in kids, body composition in adults, and a bunch of metabolic knobs clinicians take seriously because the consequences of getting it wrong can last decades.
People hear "growth hormone" and their brain goes straight to gym folklore, anti-aging clinics, and the whole "GH + IGF-1 + insulin = easy-mode gains" story. Medicine is less impressed. GH is a powerful hormone, yes, but it's also moody, pulsatile, and annoyingly hard to measure directly, which is why legitimate diagnosis leans on dynamic testing, IGF-1 levels, imaging, and actual clinical context, not vibes.
What does "GH" mean in medicine?

GH is growth hormone, a peptide hormone made by somatotroph cells in the anterior pituitary. In endocrinology, you'll also hear it called somatotropin (same idea, older physiology language), and you'll see its downstream partner everywhere: IGF-1 (insulin-like growth factor 1).
A clean way to keep the terminology straight, since clinics, insurers, and patients all use slightly different words:
-
GH: growth hormone (the hormone your pituitary secretes).
-
HGH: human growth hormone (the human form, usually used in public conversation, sometimes in prescriptions and patient-facing materials).
-
Somatropin / rHGH: manufactured recombinant human growth hormone used for treatment, with FDA-labeled indications outlined in the FDA's own page on somatropin information and approved uses.
-
IGF-1: the liver-produced mediator that carries a lot of GH's growth signal into tissues via IGF-1 receptors.
GH vs HGH
Clinically, the difference is mostly context and audience. Doctors say GH. Patients say HGH. Bodybuilding forums shout HGH. On the legitimate medical side, "HGH" often just means "human growth hormone" in plain English, not a different molecule.
Somatotropin
Somatotropin is the biologic hormone your pituitary secretes. It's part of the family of pituitary hormones, and it doesn't work like a steady drip. GH secretion comes in pulses, so a random blood draw can look "normal" even when the axis is broken.
IGF-1
If GH is the signal, IGF-1 is the receipt. GH stimulates the liver (and some local tissues) to increase IGF-1 secretion, raising serum IGF-1 concentrations. Because IGF-1 is more stable across the day than GH, it's often used as a screening and monitoring marker, especially when you're trying to make sense of low IGF-1 level versus high IGF-1 level patterns.
Where is it made and what controls release?
Anterior pituitary
GH is made in the pituitary gland, specifically the anterior lobe. It's tiny, it sits in the sella turcica, and it can cause outsized chaos when a pituitary tumor shows up or when the gland gets damaged by surgery, radiation, trauma, inflammation, or congenital issues.
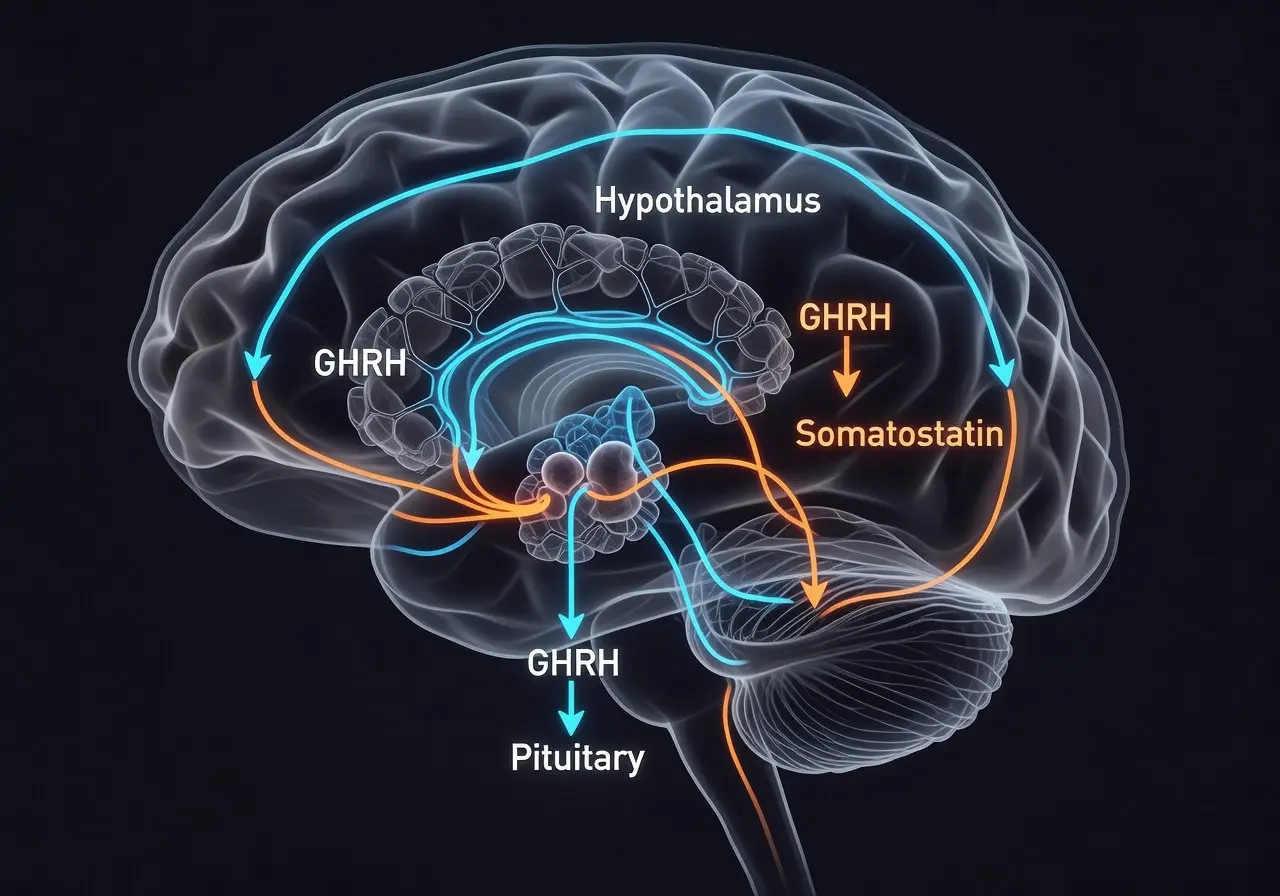
GHRH and somatostatin
The hypothalamus runs the throttle and the brake. GHRH (growth hormone–releasing hormone) tells the pituitary to secrete GH. Somatostatin tells it to stop. That tug-of-war is why GH doesn't behave like thyroid labs where you can casually draw at noon and call it a day.
If you want the physiology written out in an academic, no-nonsense way, the NCBI Bookshelf overview of growth hormone regulation and pulsatile release is one of the cleaner explanations.
Sleep, exercise, fasting
GH release tends to spike with deep sleep, exercise, and fasting, and it shifts with age, sex steroids, and body composition. That's why your friend's "I tested my GH once and it was low" story is basically useless without context. You can catch GH at a trough and convince yourself you're broken.
What does it do for growth and metabolism?

Linear growth
In kids with open growth plates, GH drives linear growth largely through the IGF-1 axis. In normal puberty, GH and sex steroids help produce the classic growth spurt. In pathologic states, you can see abnormal growth velocity as the signal something's off, sometimes alongside early puberty patterns like precocious puberty that complicate the whole picture.
Muscle and fat
This is where the internet gets loud. GH shifts body composition, often nudging fat down and lean mass up, but that does not automatically translate into "you add 50 pounds to your bench." Frankly, I'm skeptical of the mythologized version: GH/IGF-1 looks a lot like a body-composition hormone, and the human performance data people cite in comment sections is messier than the confidence level. A review on misuse patterns and what's actually shown in humans is sobering if you read it without the hype filter in place, like this analysis of performance-enhancing hormone abuse.
Glucose effects
GH can push glucose up by reducing insulin sensitivity in muscle and increasing lipolysis. It's one reason clinicians pay attention to glucose trends during GH treatment, and it's also why the "stack it with insulin" crowd is playing with something that can turn into glycemic control roulette fast. Insulin is powerful. It is also unforgiving.
What happens when levels are too low?
Pediatric signs
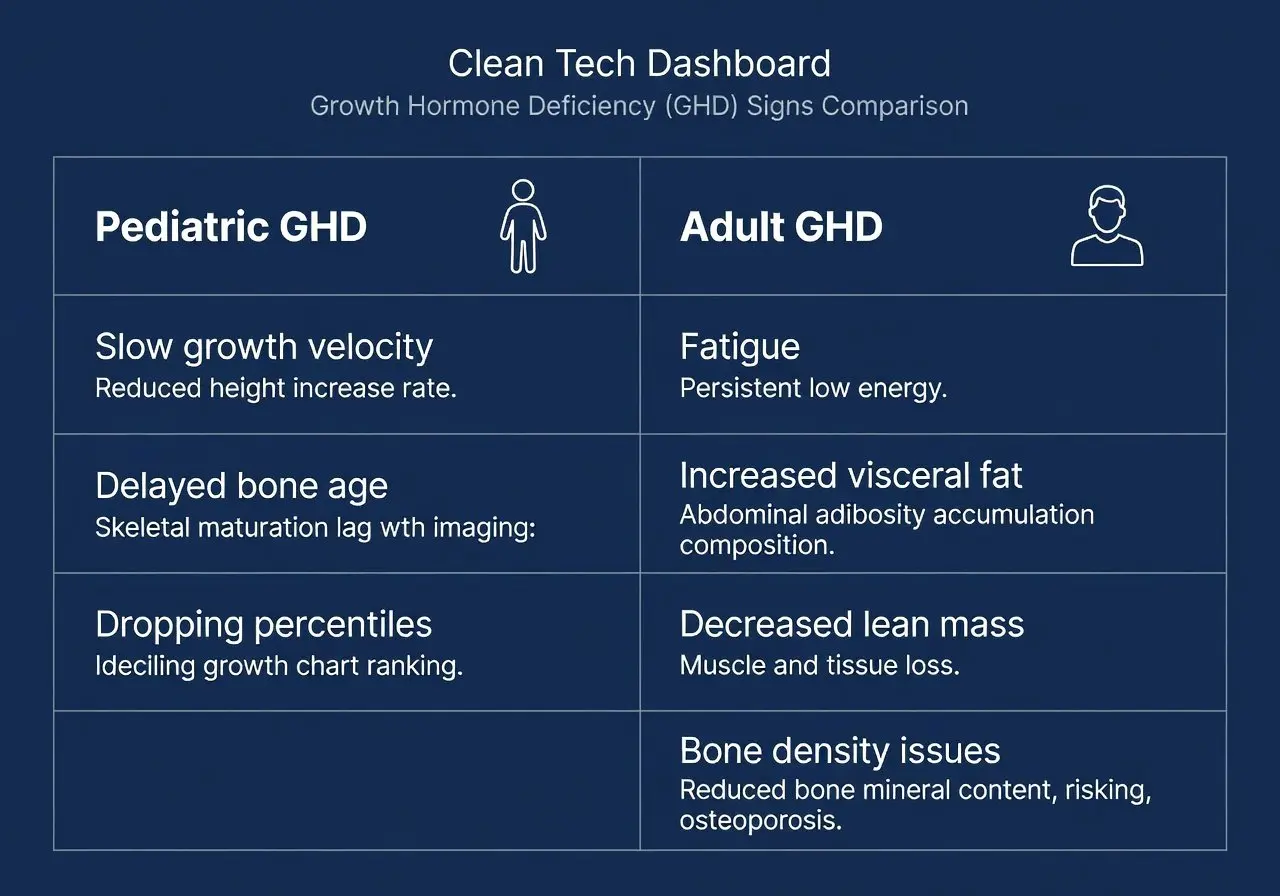
In children, growth hormone deficiency (GHD) often shows up as slow growth velocity, delayed bone age, and a kid dropping percentiles over time. It's not just "short." Some kids are short because their parents are short. The red flags are trajectory and pattern.
Adult signs
Adults can have GHD too, especially after pituitary surgery, radiation, traumatic brain injury, or true hypopituitarism. Adult GHD is less about height (obviously) and more about fatigue, reduced exercise capacity, increased visceral fat, decreased lean mass, and bone density issues. The Endocrine Society's adult GHD clinical practice guideline is basically the map clinicians use when they're being careful, which they should be.
Common causes
Causes split into "the gland can't make it" and "the system can't signal it," with pituitary adenomas, craniopharyngioma, congenital pituitary abnormalities, infiltrative disease, head trauma, and iatrogenic causes (surgery, radiation) all living on that list. In practice, you also see kids referred for short stature where the final diagnosis is not GHD at all, but something like SGA (small for gestational age without catch-up growth) or ISS (idiopathic short stature), which matters because treatment language and insurance logic changes.
What happens when levels are too high?
Pituitary adenoma
Most true GH excess is from a GH-secreting pituitary adenoma, basically somatotroph tumors pumping GH with no respect for feedback. The result is elevated GH and typically elevated IGF-1, plus a slow-motion collection of physical changes that people often normalize until a clinician puts the pattern together.
Gigantism
If GH excess happens before epiphyseal closure, you get gigantism (sometimes called pituitary gigantism). Think excessive linear growth plus soft tissue changes. It's rare, but when it happens, it's a medical emergency in the "this will reshape an entire life" sense.
Acromegaly
After growth plates close, GH excess becomes acromegaly. Hands and feet enlarge, facial bones thicken, the jaw can push forward, rings stop fitting, shoes creep up sizes. There are systemic effects too: sleep apnea, cardiomyopathy, hypertension, insulin resistance, joint disease. It's not cosmetic. It's organ-level.
Use tests and imaging to confirm a disorder
Why random levels mislead
A random GH level is often misleading because GH is secreted in pulses with a short half-life. You can draw at the wrong time and get a "normal" number in someone with disease, or a "high" number after exercise and convince yourself they have a tumor. That's why serious evaluation relies on dynamic testing and IGF-1.
Insurers actually acknowledge this biology in their criteria, like the FEPBlue policy noting the need for stimulation testing because of the hormone's rapid fluctuations, which you can see spelled out in their adult growth hormone testing requirements.
Stimulation and suppression tests
When clinicians suspect deficiency, they use a GH stimulation test. When they suspect excess, they use a GH suppression test (classically an oral glucose tolerance test where GH should suppress).
Here's the quick comparison people usually want, without pretending this replaces a real endocrine workup:
|
Clinical question |
Common approach |
What "abnormal" means in plain English |
|---|---|---|
|
Is there GH deficiency? |
Dynamic stimulation (varies by protocol) |
GH fails to rise appropriately under provocation |
|
Is there GH excess? |
Oral glucose suppression |
GH fails to suppress when it should |
Cutoffs can depend on assay, BMI, and protocol. One detailed review goes into BMI-dependent thresholds and the messiness of interpreting peaks, like this evaluation of GHD testing across ages.
IGF-1 and pituitary MRI
IGF-1 release is steadier, so serum IGF-1 concentrations are often used to screen and to monitor therapy dosing. If IGF-1 is clearly elevated and the clinical picture fits, the next step is often a pituitary MRI to look for adenomas. If IGF-1 is low and the patient's history screams pituitary injury, you still confirm with dynamic testing before calling it.
Start therapy safely and know key terms

In actual prescribing, "GH therapy" almost always means somatropin, recombinant human growth hormone given by subcutaneous injection, traditionally daily. There are now longer-acting formulations too, including weekly options. A regulatory update on somapacitan points out a real-world adherence point: a weekly injection can remove up to 313 daily injections per year, which is not nothing if you've ever tried to get a tired family to stick to nightly meds, as described in this Pharmacy Times report on expanded pediatric indications.
A few terms you'll see thrown around in notes and prior auth paperwork:
-
GHD: growth hormone deficiency (pediatric or adult).
-
SGA: small for gestational age with inadequate catch-up growth; there's an international consensus guideline that even includes dosing ranges, like the Endocrine Society's SGA guideline.
-
ISS: idiopathic short stature, a controversial bucket that often turns into an ethics and expectations conversation, not just a prescription.
Administration-wise, clinics do GH injection training, rotate sites, and monitor growth velocity (kids), symptoms and body composition (adults), and labs including IGF-1 levels. Dose is individualized, titrated, and monitored. Endocrinologists do not dose this like a supplement.
Long-term safety data is often more reassuring than people expect when therapy is appropriately prescribed and monitored. For adults, the KIMS cohort followed over 15,000 GH-treated patients for an average of 5.3 years and reported a de novo cancer incidence that stayed statistically flat, which you can read in the KIMS database cohort review. For pediatric patients, large real-world registries like NordiNet and ANSWER include tens of thousands of children and track outcomes and adverse events over years, like this pediatric safety study across 23 countries.
What are side effects, risks, and misuse concerns?
Side effects in legitimate GH replacement often look like "too much fluid" problems: edema, joint pain, carpal tunnel symptoms, tingling, headaches. In kids, clinicians watch for rare but serious issues like slipped capital femoral epiphysis, scoliosis progression, or intracranial hypertension symptoms. Glucose changes can happen, so diabetes risk gets attention, especially in predisposed patients.
The misuse side is its own universe. GH gets marketed like it's a fountain of youth or a shortcut to a new physique, and that's where people start free-styling with doses, stacking with anabolic steroids, and sometimes dragging insulin into the mix like it's just another "tool." I don't love moral panic, but I do hate lazy biology. If someone is pairing GH with insulin because a forum told them it's synergy, they're not being "advanced." They're volunteering for consequences they may not be equipped to recognize until it's messy.
FAQ
If GH is pulsatile, why test GH at all?
Because dynamic tests force the system to reveal itself. Random GH levels are noisy, stimulation and suppression protocols are designed to create interpretable patterns.
Is IGF-1 the same thing as GH?
No. GH is the pituitary hormone; IGF-1 is a downstream mediator, largely produced by the liver, reflecting the activity of the GH axis over time.
Does GH therapy mean the same thing as HGH?
In practice, yes. Clinically, the medication is usually somatropin (recombinant human growth hormone). "HGH" is common public language.
Can adults be prescribed GH?
Yes, for confirmed adult GHD and certain specific indications. It's not a casual "energy upgrade," and reputable clinicians follow guideline-based diagnosis and monitoring.
Conclusion
So, yeah: in medicine, GH = growth hormone, and everything that follows is an endocrine story about the anterior pituitary, hypothalamic control, IGF-1 signaling, and the very real difference between deficiency and excess. If you're dealing with short stature, suspected hypopituitarism, or signs of acromegaly, the winning move is boring but effective: get evaluated properly, use dynamic testing when indicated, interpret IGF-1 like an adult, image the pituitary when the pattern points there, and treat with somatropin only when the diagnosis and risk profile actually justify it.
Articles

Semaglutide and Tirzepatide are two of the most popular GLP-1-based peptides used for fat loss, appetite control, and metabolic support. This guide compares their mechanisms, weight loss potential, side effects, dosing, and overall effectiveness for body composition goals.

Trenbolone is a game-changer. It's a potent steroid. It's used for cutting. It's a powerhouse, a top-notch tool for bodybuilders. When you're on a mission to slice and dice that unwanted body fat, Trenbolone enters the picture. It marches into your routine, the epitome of effectiveness, the epitome of efficiency.

Anyone who has shot daily somatropin for more than a few weeks knows that some days the pen barely registers and other days it feels like a wasp landed in the abdominal fat.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.