


Semaglutide Vs Tirzepatide: Fat Loss Comparison Guide

If you're trying to pick between semaglutide and tirzepatide for fat loss, the cleanest honest answer is that tirzepatide usually produces more total weight loss and a bit more "momentum", while semaglutide still works extremely well and is sometimes easier to access or stay on depending on insurance, supply, and how your gut behaves. That's the decision. Everything else is just the fine print that suddenly becomes your whole life when you're the one doing weekly injections.
People want this to be a simple cage match. Winner takes all. In reality it's more like choosing which engine you want in the same car: both cut appetite, both change energy intake, both can make you stare at a plate of food and feel weirdly indifferent, and both can punish you if you eat like it's your last day on Earth.
What are these medications, and who are they for?

These are incretin therapies used for type 2 diabetes and for chronic weight management in adults with overweight or obesity, typically when BMI and weight related comorbidities put you into the "this is a medical problem now" zone. They're prescription-only for a reason. You are changing hormone signaling, not taking a cute supplement.
A practical way to think about who they're for is this: people with excess body weight who have tried the basics, understand this is long-term treatment, and can handle monitoring for side effects, labs, and the boring grown-up stuff like prior auth.
A lot of the internet acts like the only "eligibility" that matters is whether you want it badly enough. That is not how contraindications work.
-
If you have a personal or family history of medullary thyroid carcinoma or MEN2, these drugs are generally off the table.
-
If you're pregnant, trying to get pregnant, or breastfeeding, the conversation changes fast.
-
If you've had pancreatitis, significant gallbladder disease, or severe GI disease, you need an actual clinician weighing risk patients factors, not a comment thread.
Semaglutide products
Semaglutide shows up most famously as Wegovy (weight management) and Ozempic (diabetes mellitus). There's also Rybelsus, the oral version approved for diabetes, which is a different day-to-day experience and generally not the same weight loss indication as Wegovy's dosing.
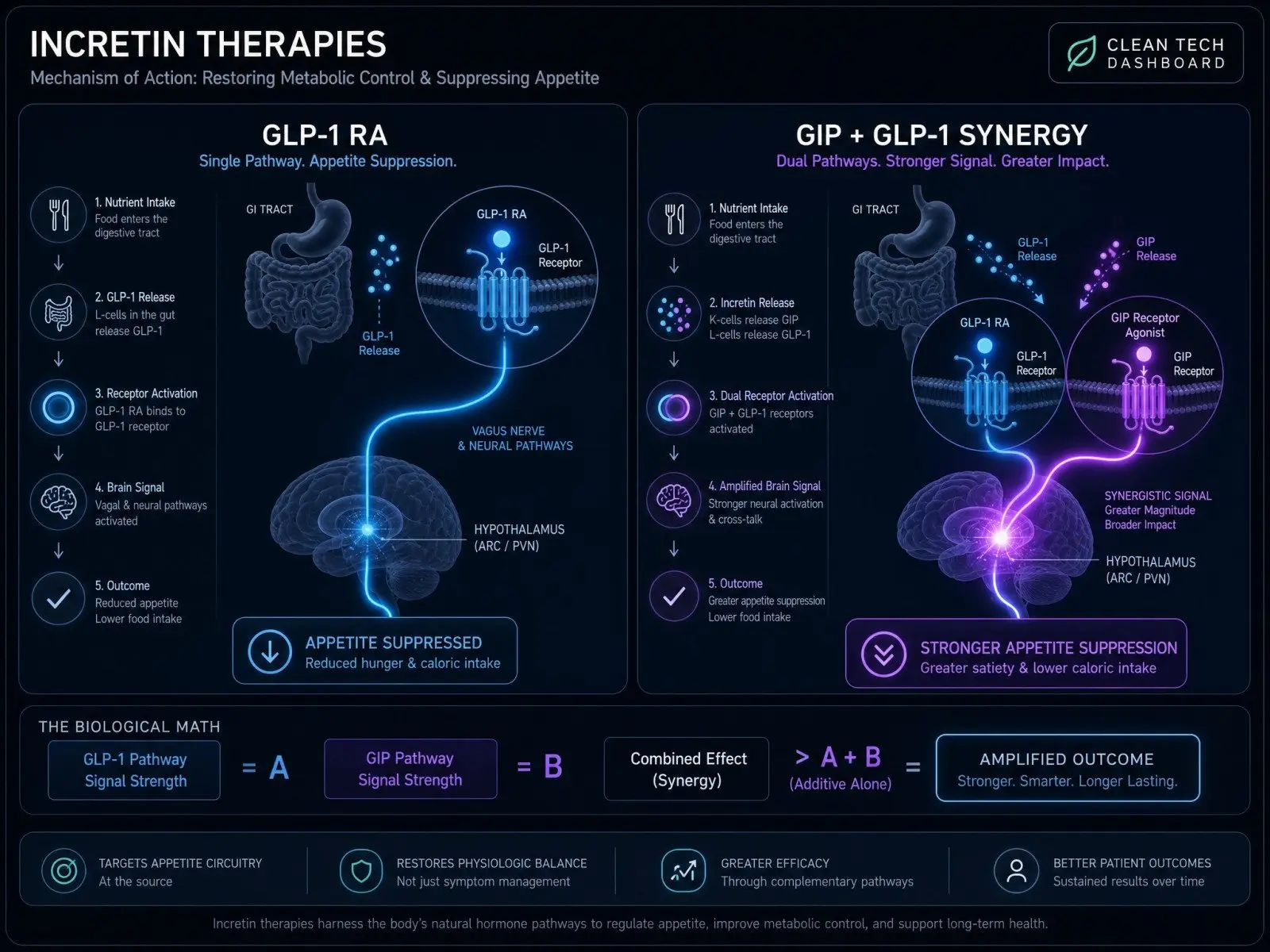
Semaglutide is a GLP-1 RA. That matters because GLP-1 signaling is doing most of the appetite and satiety work here, plus glucose control through insulin and glucagon modulation. It is also the drug with the big long-run outcomes headline lately: semaglutide's cardiovascular risk story got louder after longer-term data, including the four-year SELECT results showing sustained weight reduction and improved clinical endpoints in people with established cardiovascular disease, which is why clinicians talk about cardiometabolic disease and not just the scale when they prescribe it.
Tirzepatide products
Tirzepatide is marketed as Mounjaro for diabetes management and Zepbound for weight management, and it's a dual agonist: GLP-1 plus GIP. That extra lever is why it tends to pull harder for many people.
The best shorthand I've heard is that semaglutide often makes food quieter, while tirzepatide can make food feel like it lost its personality. Not always. But often.
Eligibility and contraindications
Most label criteria boil down to BMI thresholds plus weight related comorbidities, with documentation of baseline weight and weight history for insurance. In the real world, eligibility and "access" are different universes. Your doctor can write the glp 1 ra prescription; your plan can still say no.
Also, compounded products exist in the wild. I'm not doing the pearl-clutching thing, but be clear-eyed: compounded versions are not identical to branded products, and quality, dosing, and supply chain controls are not the same. If you're going that route, you want medical oversight and a reputable pharmacy, not a vibes-based medication request.
How do they work for fat loss?
They work mainly by changing appetite and food intake. The downstream effect is lower energy intake, which drives fat loss over time. People love to argue about metabolism like it's a mystical furnace. It's mostly math plus biology plus adherence.
GLP-1 signaling
GLP-1 receptor agonism increases satiety, reduces hunger, and slows gastric emptying, especially early in treatment. It also improves blood sugar levels via glucose-dependent insulin secretion and reduced glucagon. When people say they "forget to eat," that's appetite circuitry shifting, not willpower suddenly arriving like a superhero.
Semaglutide's track record for obesity is anchored in the STEP program, with STEP-1 showing about 14.9% mean weight loss in adults without diabetes alongside lifestyle intervention, which you can see in the published trial report in The New England Journal of Medicine describing the STEP-1 semaglutide outcomes.
GIP plus GLP-1 synergy
Tirzepatide activates both GLP-1 and GIP receptors. The why is still being mapped in endocrinol circles, but the "what you feel" is familiar: more appetite suppression for many users, strong changes in cravings, and often a bigger treatment effect on body weight change.
If you want the canonical obesity trial anchor, SURMOUNT-1 reported up to 20.9% mean weight loss at the highest dose, which is why people keep treating tirzepatide like the heavyweight champ, and the SURMOUNT-1 tirzepatide trial is the clean read.
Appetite, gastric emptying, energy intake
In the first weeks, gastric slowing can be dramatic. Later, it often attenuates, and appetite suppression becomes the more consistent driver. That's where behavior creeps back in. If your portions drift up, if your liquid calories stay sneaky, if you drink on an empty stomach and then wonder why you made nachos at 11 pm, the medication can only cover so much.
What weight-loss results should you expect?

Expected results are a range, and the range is the point. Baseline weight, dose achieved, titration pace, adherence, protein intake, sleep, alcohol, diabetes status, and plain genetics all bend the curve.
Trial averages and timelines
Most people feel "something" early. The meaningful scale change usually shows up as you climb doses. By 12 to 16 weeks, you have signal. By 6 to 12 months, you have a real pattern.
Semaglutide's STEP data commonly lands in the mid-teens percent loss for many adults without diabetes when they reach full dosing and stick with it. With diabetes, mean weight loss tends to be lower, as shown in trials like STEP-2 in The Lancet.
Tirzepatide's SURMOUNT program tends to land higher, with dose dependence that's hard to ignore. There's also the "what happens if you stop" reality, and SURMOUNT-4's withdrawal design basically underlines what clinicians already know: discontinuation often means regain.
Head-to-head outcomes
The head-to-head story is where people stop being polite. In SURMOUNT-5, tirzepatide beat semaglutide on average at 72 weeks, 20.2% vs 13.7% mean body weight reduction, and you can read the actual trial write-up in the NEJM report on the SURMOUNT-5 comparison.
Here's the simple comparison, stripped of hype:
|
Evidence snapshot |
Semaglutide (2.4 mg) |
Tirzepatide (up to 15 mg) |
|---|---|---|
|
STEP-1 mean weight loss (about 68 weeks, no diabetes) |
~14.9% |
n/a |
|
SURMOUNT-1 mean weight loss (72 weeks, no diabetes) |
n/a |
up to ~20.9% |
|
SURMOUNT-5 head-to-head mean weight loss (72 weeks) |
~13.7% |
~20.2% |
If you like real-world data, a big original investigation in JAMA Internal Medicine looked at outcomes and weight loss event probabilities, and the JAMA cohort study found higher likelihood of hitting 5%, 10%, and 15% thresholds with tirzepatide versus semaglutide in routine care, which lines up with what the trial averages suggest.
My personal bias is boring and ruthless: I care about the stronger lever. I've read enough comparisons, and watched enough people describe getting unstuck, that I'm not neutral. Tirzepatide tends to beat semaglutide on average, and even mainstream coverage of the head-to-head trial leaned that way, including reporting from Rheumatology Advisor on the trial outcome.
Real-world results and plateaus
Real-world means missed doses, travel, holidays, stress eating, supply issues, and dose caps because insurance only covers certain strengths. It also means electronic health record data that reflects messy humans, not trial participants with frequent follow-up.
Plateaus happen on both drugs. Sometimes it's true metabolic adaptation. Sometimes it's calorie creep. Sometimes you are constipated and carrying literal baggage. Sometimes your training changed and you're holding water. If the stall persists across multiple weeks with stable conditions, it's worth discussing dose escalation, adherence, or switching.
For broader perspective, pooled comparative summaries exist, and this NCBI systematic review captures the general direction clinicians keep seeing: greater weight change with tirzepatide, with broadly similar gastrointestinal adverse events rates.
What changes body fat vs lean mass?
People say "I want fat loss," then eat 900 calories and do zero strength work and act shocked when their body doesn't only burn fat like it's selecting files to delete.
Fat-loss-to-lean-loss ratios
Both drugs reduce body weight. The composition of that loss depends on protein, training, sleep, and the speed of loss. Some analyses suggest tirzepatide may have a better fat-loss-to-lean-loss ratio, meaning more fat relative to lean tissue preserved, which is part of why it's getting a reputation for better body composition outcomes in some reviews and meta-analysis work.
Still, no injectable can outsmart physics and physiology forever.
Protein and resistance training
If you want a practical north star, it's this: treat protein and resistance training as your anti-regret policy. People under-eat protein because appetite is down, then they feel weak, then their training drops, then lean mass loss accelerates.
I'm not giving you a meathead lecture, but you do want consistent resistance training and intentional protein. You also want to watch for micronutrient deficiencies, especially if your diet becomes narrow because everything feels unappealing. That "Atan D micronutrient deficiencies" rabbit hole is real for aggressive dieters, medication or not.
Rapid loss risk factors
Rapid loss tends to be riskier for lean mass, gallstones, and just feeling awful. The most common setup looks like this: high baseline weight, aggressive calorie restriction, minimal protein, minimal lifting, poor hydration, and dose increases stacked too quickly. Slow down. Your future self likes you more when you slow down.
Compare dosing, pens, and titration pace
Both are typically once-weekly subcutaneous injections with titration schedules designed to reduce side effects. In reality, titration is also an adherence tool. If you rush, you suffer, then you quit.
Weekly schedules and dose ranges
Semaglutide for weight management is commonly titrated 0.25 mg upward to 2.4 mg weekly. Tirzepatide often starts 2.5 mg weekly and titrates up through 5, 7.5, 10, 12.5, to 15 mg.
|
Practical dosing feel |
Semaglutide |
Tirzepatide |
|---|---|---|
|
Typical frequency |
Weekly |
Weekly |
|
Typical titration style |
Gradual to improve tolerability |
Gradual, with more dose steps |
|
"Ceiling" dose in obesity labeling |
2.4 mg |
15 mg |
People obsess over the pen like it's a gadget review. What matters is whether you can stay consistent week after week.
Missed dose rules
Rules vary by product labeling, so follow your specific insert, but the common pattern is a window where you can take the missed weekly dose within a few days, and if you miss beyond that you skip and resume on your scheduled day. Don't double-dose to "catch up." That's how you earn a bathroom-floor memoir.
Practical adherence tips
Most adherence problems are stupidly human: forgetting the day, being out of town, not having alcohol boundaries, eating too fast because you still think you're the old you. Put the injection day on a recurring calendar. Keep a boring routine meal option around for post-dose days. Stop treating your GI tract like it owes you.
Compare side effects, tolerability, and safety risks

Gastrointestinal side effects are the headline for both. Nausea, vomiting, diarrhea, constipation, reflux, and a sort of low-grade food aversion can show up, usually around initiation and dose increases.
A good comparative safety review exists if you want the formal language around adverse events, including thyroid and gallbladder considerations, and it's laid out in this peer-reviewed safety overview.
GI effects and mitigation
Most mitigation is not glamorous. It's portion control, slower eating, less greasy food, and hydration. People hate that advice because it sounds like the same diet advice they've heard forever. The difference is that now you can actually do it.
-
Smaller meals, more slowly, especially on dose day and the day after.
-
Prioritize protein first because you might not finish the plate.
-
Stay hydrated and manage constipation early, not after day five of suffering.
Red-flag symptoms
Some symptoms are not "normal side effects." Severe persistent abdominal pain, pain radiating to the back, jaundice, fainting, signs of dehydration that won't quit, or allergic symptoms deserve medical attention. If you have diabetes and retinopathy, vision changes matter too.
Drug interactions and special populations
Because these drugs slow gastric emptying, absorption of some oral meds can shift. If you're on insulin or sulfonylureas, hypoglycemia risk becomes a real conversation. Kidney disease, liver disease, older age, and a history of eating disorders are all contexts where your prescriber should be more cautious with dosage and titration.
Compare cost, coupons, and insurance access
This is where most "which is better?" debates die. Retail pricing is high for both drugs, coverage is inconsistent, and plans change their minds like it's a hobby.
Insurance often demands documentation: baseline weight, BMI, prior attempts, comorbidities, sometimes proof of continued response. Some people can access one but not the other. Some can only get diabetes-labeled coverage. Some hit shortages and are forced into switches they did not want.
If you're paying out of pocket, cost becomes part of tolerability in a way nobody likes to admit. Financial stress is a side effect.
Decide which fits your goals and constraints
If your goal is maximum average scale movement, tirzepatide has the edge in both clinical trials and cohort study findings. If your goal is "I want a strong option with deep long-term outcomes data, potentially better coverage, and a huge clinical footprint," semaglutide is not some consolation prize.
I tend to side with tirzepatide for results, because the effect size keeps showing up higher, and because the lived experience people report, that sense of appetite finally shutting up, matches the direction of the evidence. If you want a nerdy deep dive into comparative real-world effectiveness beyond a single trial, there's also this large meta-analysis on comparative outcomes that reinforces the same general hierarchy.
Your constraints still matter. If you can't get the drug reliably, the best medication is the one you can actually take.
Switching and "stall" scenarios to discuss
Switching happens for four reasons: coverage, supply, side effects, or a stall that won't budge. Clinicians often restart titration when switching, even if you were on a higher dose of the other drug, because tolerability is not transferable in a neat way.
If you stall on semaglutide, the conversation is usually dose optimization, adherence, and then potentially switching to tirzepatide if access allows. If you stall on tirzepatide, you still look at the basics, but you also ask whether you truly reached and maintained an effective dose and whether lifestyle support is doing anything besides existing on paper.
If you want one reality-check that nobody loves: stopping tends to mean regaining for many people unless behavior and energy balance are handled with intention, and trials like SURMOUNT-4 made that painfully obvious.
Conclusion
Semaglutide and tirzepatide both work because they reduce appetite and reshape food intake. Tirzepatide more often produces greater weight loss and higher odds of hitting big percentage milestones, including in head-to-head data like SURMOUNT-5. Semaglutide remains a powerhouse with extensive evidence, including longer-term outcomes and cardiometabolic benefits in the right populations.
Pick the drug you can access, tolerate, and stay on long enough for the math to actually play out, then protect your lean mass like it's your job. That's the part people skip, and then they blame the pen.
Articles

SERMs vs AIs: in post-cycle therapy (PCT), a SERM is usually the main engine for restarting LH/FSH and natural testosterone production, while an aromatase inhibitor is a situational tool for documented high estradiol that is actively causing problems.

Bitcoin is a digital currency that requires a Bitcoin wallet to store and use it. This guide will show you step-by-step how to create a wallet, validate it, and receive Bitcoin.

Quick answer: Cartalax (often written Cartalax AED) is an experimental short-peptide bioregulator, usually described as the tripeptide Ala-Glu-Asp, studied for cartilage support and age-related joint decline. People usually find Cartalax after hitting a wall with their knees, hips, shoulders, or hands and going hunting for the compound nobody mentioned at the orthopedic visit.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.