


GHK-Cu vs BPC-157 vs TB-500: Differences Guide For Recovery
If you've been hanging around peptide forums long enough, you've seen the same movie on repeat: someone tweaks a shoulder, gets spooked about surgery, reads a few "miracle recovery" comments, and suddenly they're comparing GHK-Cu vs BPC-157 vs TB-500 like they're choosing between running shoes.
So let's put the answer up front, cleanly: GHK-Cu is mostly a copper signaling compound used for skin remodeling and cosmetic repair; BPC-157 is a gut-derived peptide studied mostly preclinically for tissue protection and inflammatory modulation (often framed around tendons, ligaments, and GI); TB-500 is a lab-made fragment associated with thymosin beta-4 biology, typically marketed for soft-tissue recovery and cell migration, with a different evidence footprint and more sports anti-doping baggage. They're not interchangeable. They don't "heal everything." And the internet's favorite "stack for joints" vibe is, frankly, way more vibe than verified.
I'm also going to be real in the way you asked: the loudest consistent theme in user stories is not the benefits. It's tolerability. The sting, the injection misery, the anxiety-y "what is happening to my body" moments, the "copper uglies" complaints, and the classic sunk-cost line, "No results yet, staying on it a few more weeks." That doesn't prove they never work. It proves the day-to-day cost is often the most measurable part of the experiment.
What should you expect from these compounds?
Best-supported outcomes
People want one sentence promises. Biology gives you probabilities and maybes.
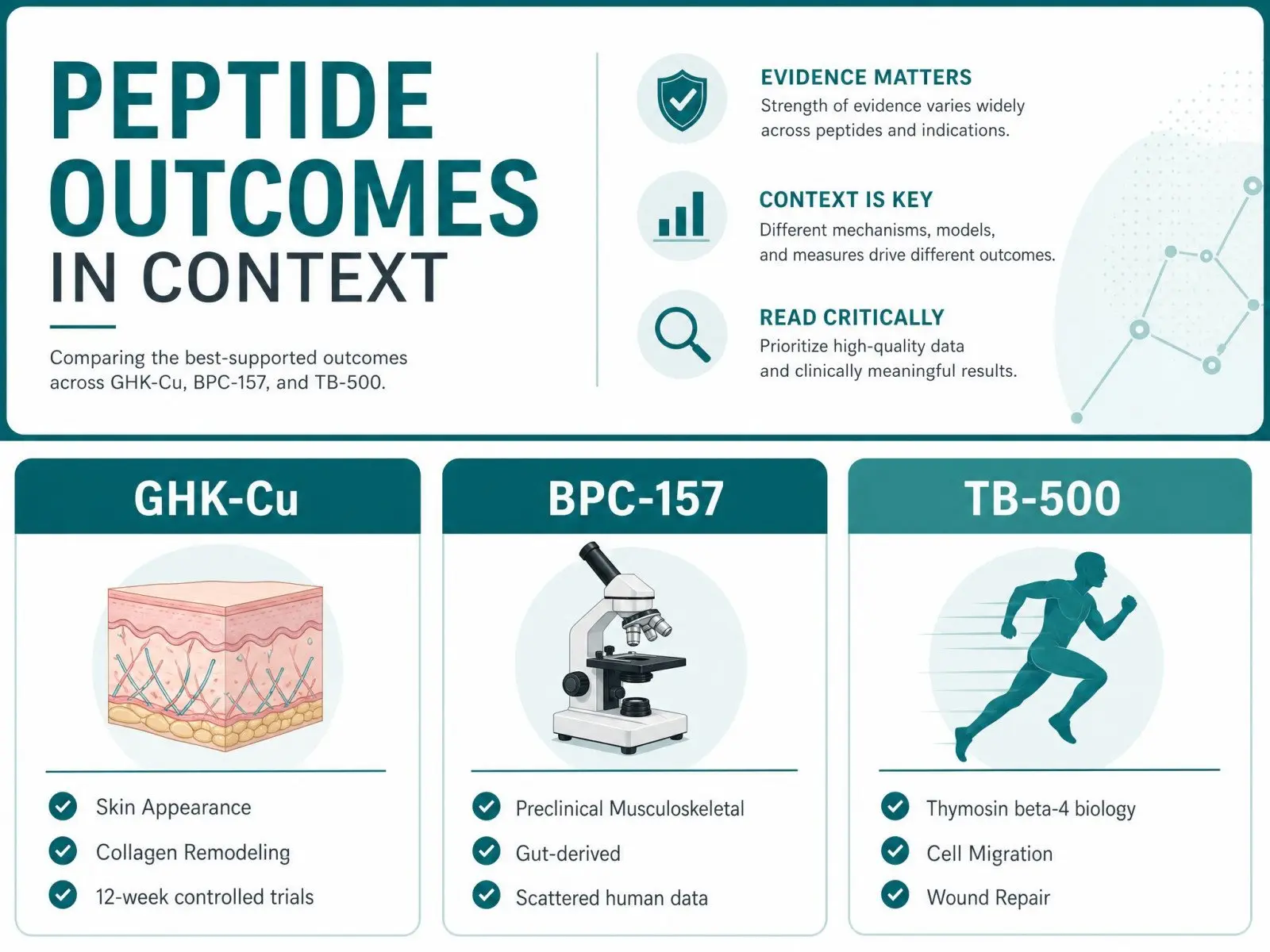
The best-supported outcomes, based on the current research landscape, tend to land like this:
- GHK-Cu has its most defensible lane in skin appearance, collagen-related remodeling, and wound context, including signals seen in a 12-week controlled trial tracking skin thickness and photoaging changes that gets cited a lot in derm circles when people want something less mystical than influencer screenshots.
- BPC-157 has a huge preclinical footprint and a scattered human footprint; a recent systematic review of musculoskeletal studies basically highlights the same tension you feel reading the forums: lots of interest, limited high-quality human endpoints.
- TB-500 / thymosin beta-4 biology has legitimate mechanistic writing around wound repair and cell movement, and the "it closes tissue faster" idea shows up in older in vivo work like the one reporting acceleration of re-epithelialization and wound contraction.
If you're expecting a fast, obvious "pain is gone" signal, you're setting yourself up for interpretation games. The body is noisy. Sleep changes pain. Training volume changes pain. Placebo changes pain. Mood changes pain. It's a whole system, not a lab dish.
Common hype patterns
This is where people get gently (or not so gently) misled.
A few patterns show up over and over:
- "Shoot it and your body fixes itself." The mechanism gets described like a magic wrench tightening loose bolts. Real healing is slower, boring, and often incomplete.
- "Stack three things so you cover all pathways." Sounds scientific. Usually turns into attribution chaos.
- "If it hurts, it's working." No. Pain can be technique, dilution, histamine-y response, contamination risk, or just you irritating tissue with repeated injections.
And yes, I'm including my own bias here: GHK-Cu injection stories are weirdly consistent about the rough experience. People spend more energy on dilution math and needle angle than on objective tracking. That's not a dunk. It's a practical warning.
Who should avoid self-experiments
If you're dealing with immune-driven disease, uncontrolled psychiatric symptoms, pregnancy, active cancer concerns, complicated liver or kidney disease, or you're mixing a dozen compounds because a subreddit said "synergy," stepping back is not cowardice. It's adult behavior.
Autoimmune conditions deserve special bluntness. Psoriatic arthritis, for example, is not a "my tendon is cranky" situation. It's systemic inflammation with immune response wiring baked in, and trying to plaster it over with unproven peptides while skipping validated medical management is the sort of gamble that feels brave right up until it isn't.
How do mechanisms differ at a high level?
GHK-Cu signaling
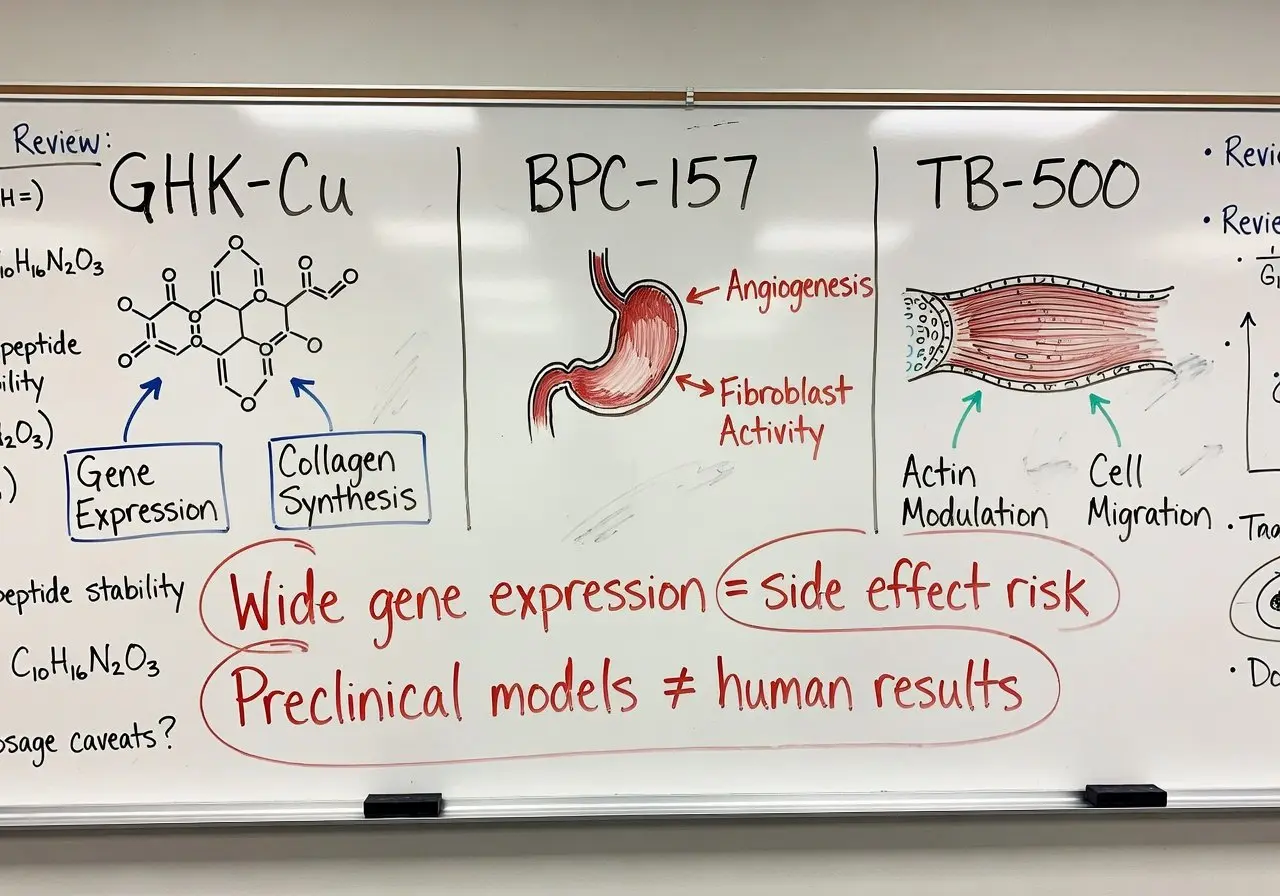
GHK-Cu is a copper complex, and copper is not a cute accessory mineral. It's enzymatically serious. The reason GHK-Cu gets so much skin attention is the remodeling conversation: collagen synthesis, extracellular matrix behavior, and the general "repair mode" signaling people summarize as skin regeneration.
One of the more eyebrow-raising pieces is how broadly it seems to tug gene expression; the paper describing large gene-expression shifts using the Broad Institute Connectivity Map gets referenced because it suggests GHK-Cu is not just "collagen lotion," it's a molecule that can change cellular behavior in a wide, messy way. Wide is not automatically good, by the way. Wide is also how you get side effects.
Also, delivery matters more than people admit. There's a reason topical formulations keep coming up, including a 14-day topical gel protocol tracking punch-biopsy wound area reduction. Skin is literally the battlefield here. You don't always need to go systemic to chase a local outcome.
BPC-157 tissue pathways
BPC-157 is commonly described as "body protection compound," pulled from gastric juice context, with a research universe that is huge in animals and thin in humans. The mechanistic talk typically orbits angiogenesis, nitric oxide balance, and tissue protection themes, plus fibroblast activity.
If you want a single doorway into the science maze, the review compiling a mountain of references on pleiotropic pharmacology is the kind of thing that makes you understand why people get excited. It reads like, "It does everything." The more honest interpretation is, "It touches a lot of pathways in models." Models are not your Saturday morning long run.
One specific mechanistic breadcrumb people cite is growth hormone receptor up-regulation in fibroblasts, which sounds spicy until you remember that "up-regulation" in a lab does not automatically become "my tendon is brand new."
TB-500 thymosin axis
TB-500 is usually discussed alongside thymosin beta-4, and this is where ambiguity matters. Thymosin beta-4 is a naturally occurring 43-amino-acid peptide; TB-500 is often sold as a synthetic fragment variant, and the sequence and fragment comparisons matter because fragments are not always functionally identical.
Mechanistically, the talking points cluster around actin modulation, cell migration, and structural repair vibes, which is why it gets marketed as a muscle repair and connective tissue helper.
Also, TB-500 has a very specific "sports testing" shadow. Anti-doping labs can detect thymosin beta peptides at extremely low levels, and the paper describing a mass spectrometry detection limit used in anti-doping verification is a reminder that WADA and USADA do not care about your "recovery protocol," they care about banned methods and analytes.
Primary targets and best-fit use cases
Skin and hair goals

If your goal is cosmetic, GHK-Cu is usually the first name people reach for, mostly because it lives comfortably in topical options and skin health conversations. There's even a historical arc here: the 1973-era discovery details on natural serum decline and antioxidant pathways are part of why it got positioned as a "youth signaling" piece in the first place.
Hair is murkier. People love before-and-after photos; lighting also loves before-and-after photos. If you're chasing hair, you should be thinking about follicles, androgen signaling, inflammatory scalp conditions, and whether you're already ignoring the boring heavy-hitters (like clinically tested options) while hoping a copper peptide turns back time.
Tendon and ligament goals
This is where BPC-157 and TB-500 get pushed hardest, especially for tendons and ligaments that heal slowly because their blood supply is limited and the rehab timeline is emotionally offensive.
BPC-157 has preclinical coverage across tendon and ligament injury models, including reviews summarizing dozens of preclinical tissue recovery protocols. That doesn't mean your elbow tendon will regenerate on a neat schedule. It means the hypothesis isn't pulled from thin air.
TB-500 gets positioned more as "global soft-tissue recovery," with people claiming it helps them tolerate training load. Cool story, but if you don't change the behavior that caused the tendon flare, you're basically using chemistry to negotiate with physics.
Gut and inflammation goals
BPC-157 has the clearest gut narrative, since it's tied to gastric stability and has long-running gastroprotective research; the paper describing decades of data on stability in human gastric juice is part of why oral and systemic conversations exist at all.
For inflammation, especially systemic inflammation, tread carefully. "Reduced inflammation" is the easiest claim to make and the hardest to verify without labs, standardized symptom scoring, and time. If your "inflammation plan" is basically vibes plus a peptide stack, you're not doing medicine, you're doing roulette with nicer packaging.
Delivery methods and protocol structure basics
Injection routes
In practice, most people doing BPC-157 or TB-500 are using subcutaneous injection, sometimes trying to go "near the injury," even though local-versus-systemic distribution is not as simple as pinning near a sore spot.
And GHK-Cu injections? This is where you hear the most complaints. The sting, the lingering irritation, the "what did I just do" regret. My take from the anecdotal swamp is blunt: if the injection experience is dominating the story, you're losing the plot. Recovery is not supposed to become a daily pain ritual.
Topical options
Topical GHK-Cu is the least chaotic entry point for a lot of people because it matches the target tissue. If the goal is scar appearance or skin regeneration, topical delivery is at least coherent. It's also easier to stop if you react poorly.
TB-500 and BPC-157 topicals exist in the marketplace, but the evidence and absorption assumptions tend to be shakier. You're often paying for hope and a nice label.
Cycle and tracking
![]()
Most "protocols" you see online are folklore, not clinically standardized dosing. If you do anything anyway, tracking is your only defense against self-deception: pain scale, range of motion, training volume, sleep, resting heart rate, maybe CRP if you're actually working with a clinic.
People hate this part. They want the vial to be the plan. It's not.
When should you choose one over another?
Acute injury scenarios
Acute sports injury care is about reducing aggravation, restoring function, and not turning a strain into a six-month saga. In that context, the "pick" is less about which peptide sounds coolest and more about whether you've already nailed the unsexy basics: imaging if needed, physical therapy, load management, and a real diagnosis.
If someone is dead set on experimenting under medical supervision, BPC-157 is the one most often matched to acute soft-tissue injury narratives, mostly because of its tissue protection framing. TB-500 shows up too, but it comes with more regulatory and sports eligibility risk if you're competing.
Chronic pain scenarios
Chronic pain is where these compounds get misused as emotional relief. People want a switch flipped.
If pain is chronic and multi-factorial, and you have central sensitization, poor sleep, job stress, autoimmune disease, or metabolic issues, you're not choosing a peptide, you're choosing whether to build a treatment plan that respects the whole body. That may include regenerative medicine consults, sure, but it should also include diagnostics and boring consistency.
Cosmetic and scar scenarios
This is GHK-Cu's most coherent lane. Skin remodeling, collagen, appearance, post-procedure support, and surgical healing aesthetics are where it fits the story best, especially topically.
If you're injecting GHK-Cu purely for "glow," and the main effect you notice is discomfort or weird side effects, you're allowed to call it. That's not quitting. That's reading the room.
Stacking rules, synergy claims, and attribution problems
Why stacks feel convincing
Stacking feels like you're being thorough. Complementary mechanisms, synergistic healing, cover all bases, hit inflammation and repair and collagen synthesis at once. It scratches the same itch as buying every supplement at the fitness center 340 s whitney way because you're fired up and you want a shortcut.
My issue is simple: stacks destroy signal. If you feel better, you can't tell what helped. If you feel worse, you don't know what to stop. The "tb 500 stack" culture is basically built to generate stories, not clarity.
How to isolate effects
You isolate by being annoyingly strict. One change at a time. Same training plan. Same rehab work. Same sleep targets. Track for long enough that random good days don't trick you.
If you're working with a medical wellness center, this is the part where a cautious provider earns their money: they slow you down.
When stacking raises risk
More compounds means more variables: contamination risk, dosing errors, unexpected immune response, anxiety spikes, blood pressure weirdness, interactions with other therapies, and just plain decision fatigue.
And please, do not ignore regulation. The FDA has not approved BPC-157 or TB-500 for general therapeutic use, and product potency in gray markets is not a vibe, it's a safety problem. Athletes also need to keep WADA and USADA rules in mind, because "my clinic told me" is not a defense when you fail a test.
FAQ
Are these peptides FDA-approved drugs?
Generally, no for BPC-157 and TB-500 in typical retail peptide form, and GHK-Cu is more often encountered in cosmetic or topical products rather than as an approved regenerative injection drug. If someone is selling certainty here, be skeptical.
Is TB-500 the same thing as thymosin beta-4?
Not exactly. Thymosin beta-4 is a natural 43-amino-acid peptide; TB-500 is commonly sold as a synthetic fragment variant, and that distinction matters for both biology and interpretation.
Can BPC-157 help psoriatic arthritis?
Psoriatic arthritis is immune-driven. Betting on an unproven peptide as your main strategy is risky. If you experiment at all, it should be framed as an experiment with a medical provider, not a replacement for validated care.
What's the safest way to approach any of this?
Medical supervision, clean sourcing through legitimate channels, and objective tracking. Also, a willingness to stop if the "cost" is higher than the benefits.
Conclusion
If you strip away the marketing glitter, the differences are pretty grounded: GHK-Cu is the skin-and-remodeling signaler with copper biology behind it, BPC-157 is the preclinical darling with gut roots and broad tissue-protection claims, and TB-500 is the actin-and-cell-movement flavored recovery molecule with extra anti-doping and identity confusion attached.
The contrarian truth I keep coming back to is annoyingly human: most people don't fail because they picked the "wrong peptide." They fail because they tried to outsource patience. They skipped rehab. They didn't track anything. They stacked three compounds, felt a weird sensation, called it progress, and then got stuck chasing the story instead of the outcome.
If you do decide to engage with peptide therapy, do it like an adult with a plan, not like a gambler with a vial. And if a clinician like dr stephen matta (or whoever you trust locally) slows you down and asks for labs and tracking, that's not gatekeeping. That's what real support looks like.
Articles

BitCoins is one of new e-payments methods. Bitcoin purchases are discrete. Bitcoin transactions are never associated personal identity and cannot be traced.

SERMs vs AIs: in post-cycle therapy (PCT), a SERM is usually the main engine for restarting LH/FSH and natural testosterone production, while an aromatase inhibitor is a situational tool for documented high estradiol that is actively causing problems.

The choices made for a Cutting cycle is between two popular steroids: Turinabol vs Anavar. The right steroid can accelerate your journey towards ripped muscles, but the wrong one? It can derail your progress, or worse, endanger your health. Choosing becomes vital.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.