


Exemestane Vs Anastrozole: PCT Gynecomastia Risk Guide
Exemestane Vs Anastrozole
For PCT gynecomastia risk, exemestane tends to be the safer bet than anastrozole when you're worried about estrogen rebound after you stop, because it permanently inactivates aromatase instead of temporarily blocking it. That doesn't mean it's "better" for every human body or every post cycle therapy situation. It means the failure mode is different, and in PCT, failure modes matter.
People get cute online and talk about estrogen like it's a single knob you turn left or right. Then they wonder why their nipples are screaming two weeks later. Estrogen management is one of the main levers that affects PCT outcomes, breast pain, and that miserable gray zone where testosterone recovery is trying to wake up while your hormones are still acting like they're on a steroid cycle.
If you're reading this because you're trying to "reverse" gyno with a couple of pills and a prayer, I'm going to be annoying and honest: you can often calm the active phase, tenderness, swelling, and puffiness, but established glandular tissue doesn't always vanish. People confuse "less inflamed" with "gone." Those are different realities.
How estrogen control changes PCT and gyno odds

Aromatase and estradiol
Aromatase is the enzyme that converts androgens into estrogens. In men, that conversion is normal physiology, not a design flaw. During steroid use or exogenous testosterone, aromatase activity can climb in a way that spikes estrogen levels relative to your own baseline. That shift is why so many enhanced bodybuilding stories sound the same: water retention, mood swings, libido weirdness, fat gain, and sometimes that unmistakable nipple sensitivity that makes you stand in the shower doing mental math.
Clinically, third-generation aromatase inhibitors can meaningfully drop the estradiol to testosterone ratio in males, which is part of why they show up in male endocrinology discussions at all, not just breast cancer care. The catch is that "drop" is easy. Landing in a usable estrogen balance is the hard part.
Breast tissue triggers
Gynecomastia risk is mostly about estrogen signaling in breast tissue outcompeting local androgenic support. That can happen with high estrogen, with high individual estrogen sensitivity, and sometimes with rapid swings that make the tissue feel like it's being poked with a live wire. The early "active" phase tends to be the window where symptom control is most realistic.
A thing people hate hearing: if you're months or years in and the tissue feels fibrous, you're not negotiating with a fresh hormonal flare-up anymore. You're negotiating with biology that already remodeled itself. You might reduce breast events like tenderness and swelling, but the "hard lump" can stick around like an uninvited guest who brought a suitcase.
Recovery trade-offs
PCT is supposed to support testosterone recovery, not create a hormonal disaster. When you slam an aromatase inhibitor and chase minimal estrogen, you can sabotage the exact recovery you claim you're trying to protect. Low estrogen levels can come with joint pain, low libido, flat mood, sleep issues, and a general "why do I feel 80" vibe that people misinterpret as low testosterone, so they panic and start stacking more interventions.
That's the messy trade: managing estrogenic side effects without crushing the hormonal environment that makes natural testosterone production possible.
How each drug lowers estrogen
Irreversible enzyme bind
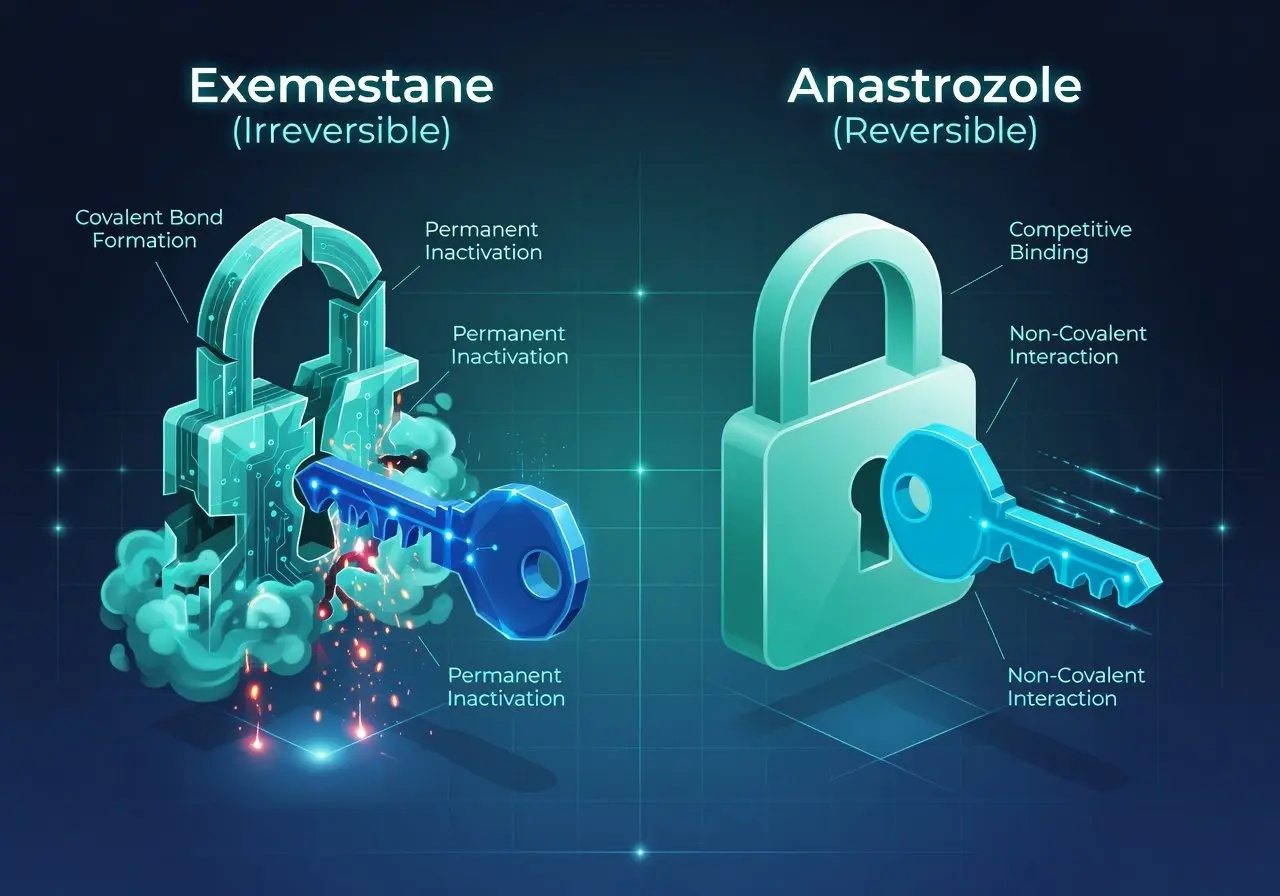
Exemestane is a steroidal aromatase inhibitor. It's structurally similar to androstenedione and works as a "suicide" inhibitor, meaning it binds to the aromatase enzyme and inactivates it. Your body has to synthesize new aromatase to restore estrogen production.
That one detail is why so many steroid users lean on it for cycle estrogen management when they're terrified of estrogen rebound. The logic is simple. If the enzyme is knocked out, you cannot immediately "bounce" back just because you stopped swallowing pills.
The FDA labeling for Aromasin spells out the basics of that clinical profile in plain language if you want the official framing, not the locker-room version, and it matters that it's positioned differently than nonsteroidal options in real prescribing practice (like after failure of another class) in the breast cancer context: the prescribing information for exemestane is worth reading once in your life.
Reversible enzyme block
Anastrozole is nonsteroidal and competitively inhibits aromatase. It sits in the active site and blocks conversion while it's present, then steps aside when it's gone. That's not "worse," it's just more reversible.
Reversibility is why you can see quick shifts in serum estrogen after dose changes, missed doses, or discontinuation. For someone who's prone to rapid swings and estrogen sensitivity, that can be a problem. For someone who wants finer, more responsive control, it can be a feature.
The FDA label for anastrozole makes the nonsteroidal, reversible mechanism pretty explicit, and yes, people in bodybuilding forums still manage to argue with the molecule like it's an opinion.
Dose-response basics
Both drugs can suppress estrogen hard. Too hard. Clinical comparisons in oncology settings have found broadly comparable effectiveness on estrogen suppression outcomes, and the MA.27 trial is often mentioned for showing no meaningful winner in major endpoints. If you want the high-level read without forum mythology, the MA.27 coverage is a clean starting point.
PCT reality, though, is not "major endpoints." It's symptom control plus not wrecking recovery.
Here's the simplest way I think about it: the more aggressively you suppress estrogen, the more likely you are to pay for it somewhere else. Lipids. Mood. Sex drive. Training quality. Sometimes all of it.
Which option lowers rebound risk after stopping
Enzyme turnover timing
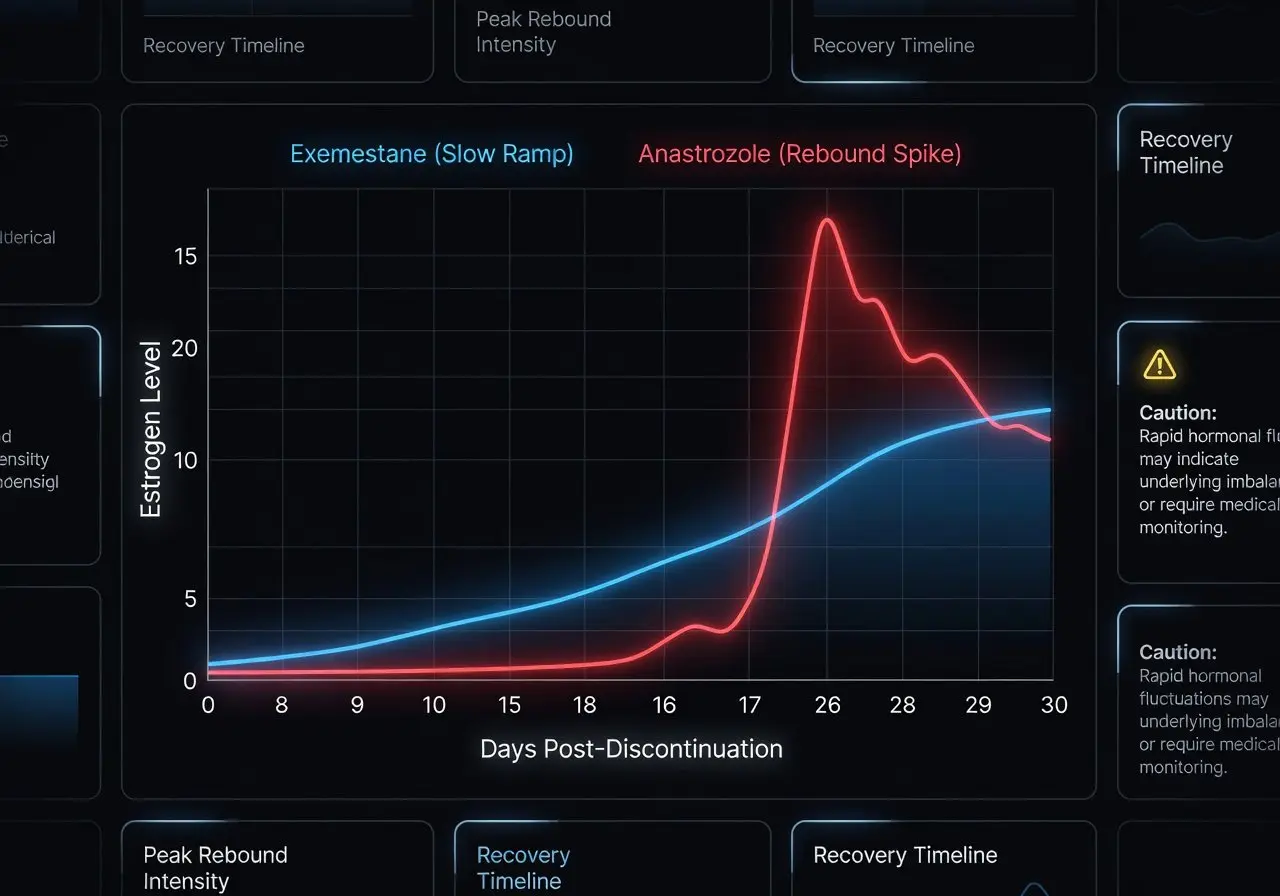
Exemestane's "suicidal" binding generally lowers estrogen rebound risk because you need new aromatase enzyme before estrogen production returns to prior levels. That makes discontinuation less like stepping off a curb and more like walking down a ramp.
Anastrozole, being reversible, can allow estrogen to climb faster after stopping. If you are finishing PCT and you pull the AI away abruptly, that climb can coincide with your own testosterone production still being shaky. That is a classic setup for gyno onset symptoms in people who are already primed.
There's a decent mechanistic discussion around reversible inhibition and rebound patterns in endocrinology literature, and the broader pharmacology of suicide inhibition is covered well in reviews like this overview on irreversible vs reversible aromatase inhibition.
Missed dose effects
Miss a dose of anastrozole and you can feel like your body is "different" in a hurry, especially if you're the kind of person whose estrogen load shows up as breast pain first and everything else second. Miss a dose of exemestane and, in theory, the impact is blunted because the enzyme population is already reduced.
"In theory" matters. People are not petri dishes. Metabolism, adherence, alcohol intake, body fat, and compound choice in anabolic steroids all change the shape of the problem.
High-aromatization scenarios
If you're coming off a cycle that had high aromatization baked in, or you're sitting at a higher body fat percentage (fat tissue expresses aromatase), rebound dynamics get louder. That's where exemestane's mechanism is attractive.
That's also where people do the dumbest thing: they keep escalating aromatase inhibitors instead of asking why the cycle estrogen management was chaotic in the first place.
Choose based on symptoms and estradiol labs
High estradiol signs
High estrogen levels in men are not one look. It's patterns. Water retention, emotional volatility, nipple sensitivity, stubborn fat gain, maybe libido swings, sometimes blood pressure changes. Some people get breast events early. Some people just get moody and puffy and deny it like it's a personality trait.
If you want a quick self-check without spiraling, these are the symptom clusters that tend to line up with elevated estrogen more often than not:
-
nipple tenderness or breast pain that's new or escalating
-
rapid water retention and "soft" look changes
-
mood swings that feel out of proportion to your life
-
libido changes paired with a puffy, inflamed feeling
Low estradiol signs
Low estrogen is its own special misery. Dry joints, flat mood, low libido, sleep fragmentation, and a general loss of training "bounce." People also report hot flashes more than you'd expect, which sounds like a joke until it isn't.
This is where my hot take about anastrozole lands: it's not that it's evil. It's that it's easy to overshoot, then you're stuck chasing how you feel with more tweaks, more "estrogen blockers," more self-experimentation, more noise.
Lab-driven decision rules
Labs should referee this, but only if you stop treating labs like a slot machine.
Here's a practical selection frame that doesn't pretend you're a robot:
|
Situation |
What it usually suggests |
Lean (cautiously) toward |
|---|---|---|
|
Active nipple tenderness plus clearly high E2 on a sensitive test |
Estrogen-driven tissue activation risk |
SERM first, AI only if labs justify |
|
History of rebound symptoms when discontinuing |
Rebound-prone pattern |
Exemestane mechanism may be safer |
|
Joint pain, low libido, flattened mood with "normal" or low E2 |
Over-suppression |
Back off AI, reassess timing and assays |
|
Normal E2 but symptoms screaming |
Could be sensitivity, prolactin/progestogenic factors, or not-gyno |
Don't escalate AI blindly |
And yes, SERMs matter here. Tamoxifen is a selective estrogen receptor modulator that blocks estrogen receptors in breast tissue, which is why it shows up in prevention and early intervention conversations more than AIs do. In fact, there's clinical research suggesting tamoxifen can outperform anastrozole for prevention of certain drug-induced gynecomastia patterns, which should make any "AI solves everything" person pause and blink twice: see this comparison of tamoxifen vs anastrozole for gynecomastia prevention.
Use AIs and SERMs safely across cycle and PCT
On-cycle roles
On-cycle, an aromatase inhibitor is sometimes used to manage estrogenic side effects from aromatizing compounds, particularly testosterone enanthate style setups where estrogen production ramps and you're trying not to bloat into a different species.
A SERM on-cycle is a different conversation and usually not the first lever for simple estrogen control, because SERMs don't lower estrogen levels, they block receptors in certain tissues.
People blur this distinction constantly. It matters.
PCT roles
During PCT, your priorities shift. You want to support testosterone recovery and avoid swinging estrogen ratios. SERMs are typically the backbone because they work at the hypothalamus and pituitary signaling level and block estrogen receptors where you actually care about gyno risk.
AIs during PCT can be justified if your actual estrogen levels are truly high and symptomatic, but the bar should be higher than "I'm anxious." Anxiety is not a lab.
When to avoid AIs
If you are already dealing with low testosterone feelings, crushed libido, joint issues, or you have labs that suggest you're not swimming in excess estrogen, pushing an aromatase inhibitor post-cycle can slow recovery and make you feel worse, not better.
Also, if you're in the "I want to reverse gyno" mindset, be careful with your expectations. This is where my skepticism comes in hard: people chase tissue reversal like it's a coupon code. Sometimes you calm the active part and the puffiness drops. Sometimes you are left with a nodule that just… exists. That reality is why surgery remains the definitive option for long-standing glandular gynecomastia.
Get estradiol testing right before dose changes

Sensitive assay choice
Most guys who think they have "normal estradiol" have never run the right test. You want a sensitive estradiol assay, often called LC-MS/MS in many lab systems, because standard estradiol immunoassays can be inaccurate at the lower ranges seen in men.
Run the correct estradiol assay or don't pretend you're making data-driven decisions.
Timing and confounders
Timing matters. Don't test the morning after you did something extreme, like a big alcohol night, a massive sodium swing, or random supplement changes. Give it consistent conditions. If you're changing doses, don't test too soon and then react to noise.
Also remember: body fat, inflammation, and liver metabolism can shift estrogen metabolism. A single number doesn't capture the whole hormonal balance, but it beats guessing.
Targets and red flags
I'm not going to hand you a magic number target because labs differ and context matters, and pretending otherwise is how people crash into low estrogen levels and then "fix" it by doing something worse.
Red flags are more useful: crashing mood, low libido, joint pain, and hot flashes after escalating an AI, especially when free testosterone and total testosterone are not recovering the way you expected.
Common mistakes that worsen outcomes
People get into trouble with the same handful of behaviors, over and over, across bodybuilders, casual steroid user types, and even folks who swear they're being "clinical" about it.
-
Treating aromatase inhibitors like estrogen blockers for feelings, not for measured estrogen levels.
-
Chasing symptoms with dose changes every few days, guaranteeing hormone swings.
-
Ignoring that tamoxifen and other SERMs are often more relevant to breast tissue than an AI, especially in early gyno prevention conversations.
-
Using the wrong estradiol test, then making confident decisions off a shaky number.
And the bonus mistake nobody admits: trying to fix everything at once. Training, sleep, PCT drugs, supplements, diet, alcohol, stress. You cannot debug a system while rewriting the entire codebase.
FAQ
Does exemestane "prevent gyno" better than anastrozole in PCT?
Exemestane's irreversible aromatase binding can reduce estrogen rebound risk after stopping, which can matter in PCT. For direct breast-tissue protection, a SERM like tamoxifen is often more targeted.
Can anastrozole cause rebound gyno after PCT?
It can, in the sense that reversible inhibition allows estrogen to rise faster after discontinuation, and that rise can collide with unstable recovery and trigger symptoms in susceptible people.
If my nipples hurt, should I immediately take an AI?
Not automatically. Nipple tenderness can reflect estrogen sensitivity, fluctuating estrogen, or other hormone dynamics. The safest move is to confirm with a sensitive estradiol test and consider a SERM-based approach for breast tissue symptoms under medical supervision.
Is "gyno reversal" realistic with drugs?
Sometimes symptom improvement is realistic, especially early. Full disappearance of established glandular tissue is not guaranteed, and pretending otherwise is how people waste months chasing protocols.
Conclusion
Exemestane vs anastrozole for PCT gynecomastia risk is mostly a debate about rebound dynamics and control style, not about which pill is "stronger." Exemestane tends to win the rebound argument because of irreversible enzyme inactivation. Anastrozole can work fine, but it's easier to whip your estrogen around and pay for it with side effects or a post-discontinuation surge.
If you want the least chaotic path, stop guessing, stop chasing "minimal estrogen," use the right estradiol testing, and treat SERMs and aromatase inhibitors like different tools for different jobs, not interchangeable fixes. And if you're already deep into long-standing gyno, be honest about what drugs can and cannot do. They're chemistry, not magic.
Articles

Sermorelin is a growth hormone-releasing hormone (GHRH) peptide that stimulates the body’s natural GH production instead of supplying synthetic HGH directly. This guide explains Sermorelin benefits, dosage protocols, recovery effects, sleep support, side effects, and safety considerations.

GHK-Cu, BPC-157 and TB-500 are among the most discussed recovery peptides, but each works through different mechanisms. This guide compares their potential benefits for tissue repair, inflammation support, recovery and healing while highlighting key differences and safety considerations.
 in Boldenone Undecylenate Cycles")
Boldenone, known more commonly as Equipoise or EQ, this anabolic androgenic steroid is a favorite among those looking to enhance their performance or achieve significant muscle growth. But, like all steroids, Equipoise comes with its own potential side effects. In fact, it can suppress your body's natural testosterone production. That's where post-cycle therapy (PCT) comes in.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.