


Comparing Clomiphene, Raloxifene and Enclomiphene for Post-Cycle Balance
It is very easy to lump these three drugs together, especially when you are tired, flat, and trying to claw your way back to normal after a suppressive cycle.
That shortcut causes a lot of bad decisions.
For post-cycle balance, clomiphene and enclomiphene usually make more sense when your main goal is restoring LH and FSH signaling, because they work upstream on estrogen feedback at the hypothalamus and pituitary. Raloxifene is different. It is more strongly valued for tissue-selective estrogen blockade in places like breast tissue and bone, with a much weaker case as a primary tool for restarting the hypothalamic-pituitary-gonadal axis.
So yes, they are all SERMs. No, they are not interchangeable.
And one more point, because internet lore gets sloppy fast. A SERM does not lower estrogen the way an aromatase inhibitor does. It changes how estrogen receptors behave in specific tissues. That means your serum estradiol can stay the same while your breast tissue, bone, liver, brain, or pituitary gets a very different signal.
This article is about clomiphene, enclomiphene, and raloxifene in a post-cycle context, not tamoxifen, not bazedoxifene, and not menopause therapy in general. Some of the tissue science comes from oncology and women's health research because that is where the receptor biology was mapped in detail. The practical question, though, is your question: if you are evaluating options for PCT, what really separates these three?
What sets these three apart?
People usually assume the answer is "strength."
It is not that simple. The split comes from receptor behavior, molecular shape, isomer content, and what tissue you actually care about.
A fast way to frame it looks like this:
|
Drug |
Core identity |
Main PCT-style appeal |
Main limitation |
|---|---|---|---|
|
Clomiphene |
Mixed-isomer triphenylethylene SERM |
Commonly used to raise LH, FSH, and testosterone |
Mixed signaling from enclomiphene plus zuclomiphene can feel less predictable |
|
Enclomiphene |
Purified trans isomer of clomiphene |
Cleaner theoretical fit for restoring axis output |
Less long-term real-world history than clomiphene |
|
Raloxifene |
Benzothiophene SERM with stronger peripheral selectivity |
Often discussed when breast tissue symptoms matter |
Less direct evidence as a primary restart agent for LH and FSH |
That table is the bird's-eye view. The real story is lower down in the weeds.
Receptor targets
All three drugs bind estrogen receptors. Specifically, they interact with ER alpha and ER beta, both part of the nuclear receptor family. But binding alone is not the whole game. If it were, every SERM would behave like a copy of the next one, and they plainly do not.
Clomiphene and enclomiphene matter in PCT talk because they interfere with estrogen's negative feedback in the hypothalamus and pituitary. When that feedback is blocked, your brain is more willing to send gonadotropin-releasing hormone, then LH and FSH, and then your testes may start producing more testosterone and supporting spermatogenesis again.
Raloxifene can also interact with those same receptors, but its reputation comes from a different pattern. It behaves as an antagonist in breast and uterine tissue while keeping more estrogen-like effects in bone. That is why it sits naturally in osteoporosis and breast risk-reduction discussions, and only secondarily in PCT forums.
Isomer status
This is where clomiphene and enclomiphene stop looking like twins.
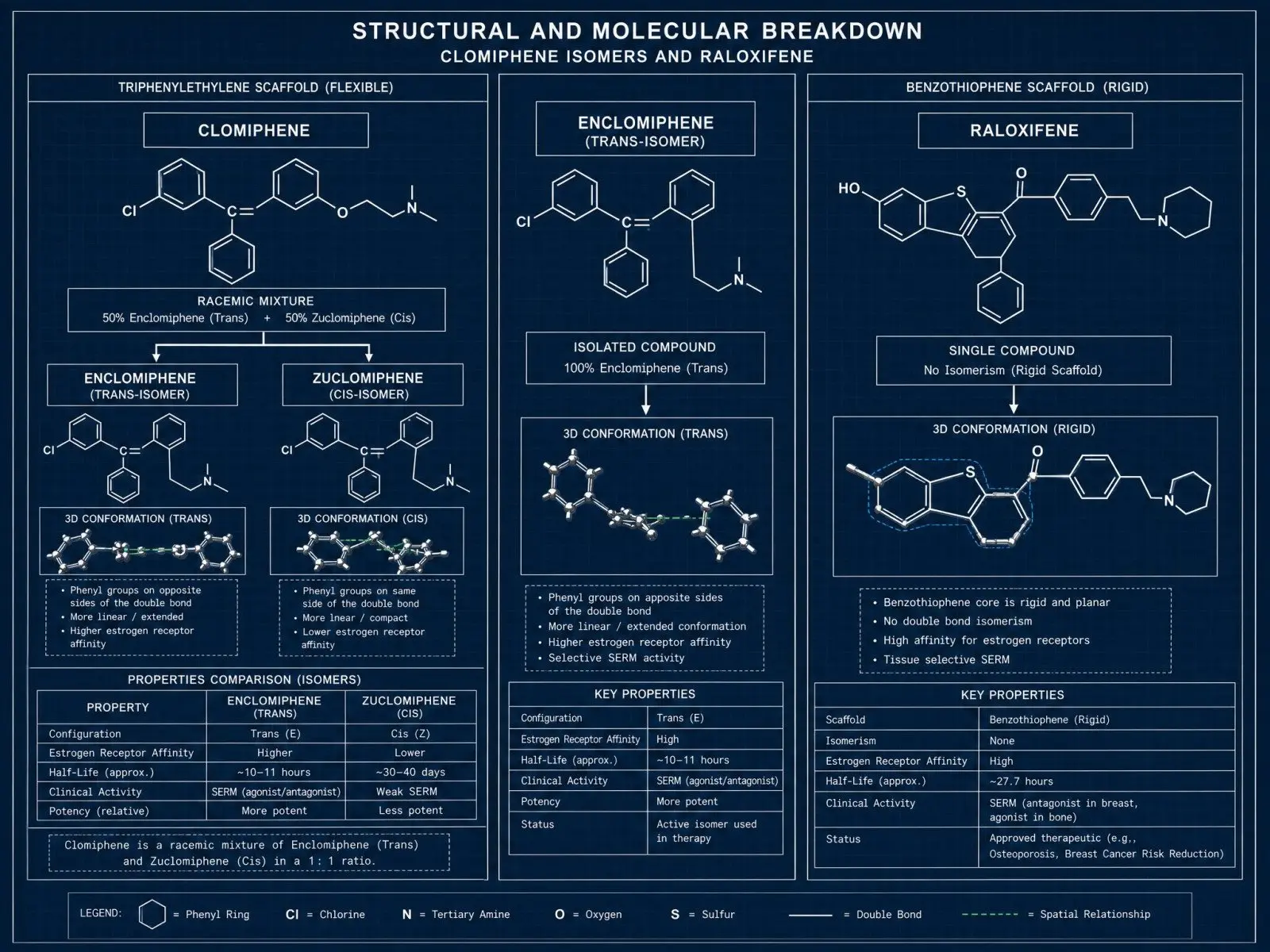
Clomiphene citrate is a mixture. Its two major stereoisomers are enclomiphene and zuclomiphene. Enclomiphene is the trans isomer and is generally associated with the more antiestrogenic, axis-stimulating effect people want in male secondary hypogonadism or post-cycle recovery. Zuclomiphene is the cis isomer and has more prolonged, partly estrogenic behavior.
That mixed-isomer reality matters. Quite a bit, honestly.
When you take clomiphene, you are not taking a single clean signal. You are taking a package deal. One part is doing much of the work you wanted, and the other part may linger longer and pull the physiology in a fuzzier direction. Enclomiphene, used as a standalone drug candidate, is basically the attempt to keep the useful half and ditch the extra baggage.
Raloxifene does not have this identity problem. It is a distinct single molecule, not a mixed-isomer fertility-era compound repurposed for male endocrine use.
Clinical role
Approved use and practical use are not always the same thing. Medicine is messy. Endocrinology even more so.
Clomiphene is officially known for ovulation induction in women, yet many clinicians have used it off-label in men with secondary hypogonadism because it can increase endogenous testosterone without shutting down fertility the way exogenous testosterone often does.
Enclomiphene was developed to sharpen that same idea. In men, the attraction is obvious: boost LH and FSH, raise testosterone, and preserve or improve sperm production rather than crush it.
Raloxifene lives in another lane. Its approved roles center on osteoporosis prevention or treatment and reduction of invasive breast cancer risk in certain postmenopausal women. In PCT circles, people talk about it mostly when nipple sensitivity or gynecomastia is the pressing issue. That is not the same as saying it is the best drug for restoring the axis. It usually is not.
How do they act at receptors?
This is the part that gets flattened into nonsense online. People say "it blocks estrogen." Fine, sort of, in a crude way. But the receptor biology is much more specific than that.
As a review on estrogen receptor conformations and coregulator dynamics makes clear, SERMs are shape-changers in the most literal receptor sense. They bind the ligand-binding domain, alter receptor conformation, and then change which coactivators or corepressors the receptor recruits. That is why the same drug can look antagonistic in one tissue and partly agonistic in another.
ER alpha
ER alpha is the big player in a lot of the classical estrogen feedback that matters for post-cycle recovery.
In the hypothalamus and pituitary, estradiol acting through ER alpha helps tell your brain there is enough sex steroid on board. When that signal is strong, LH and FSH fall. Clomiphene and enclomiphene push against that feedback. Your brain "hears" less estrogenic signaling than is actually present, so gonadotropin output rises.
This is why clomiphene can raise testosterone even though it is not testosterone.
Enclomiphene appears to do this job in a more focused way because it isolates the isomer most associated with antiestrogenic central action. In plain English, you are trying to move the command center, not just mop up downstream symptoms.
Raloxifene binds ER alpha too, but its practical reputation is less about central gonadotropin rescue and more about what happens in peripheral tissues. That makes it useful in a narrower PCT scenario, especially where breast tissue concerns are louder than low LH and FSH.
ER beta
ER beta complicates the story in a good way.
Different tissues express different mixes of ER alpha and ER beta, and they do not always read the same ligand the same way. Some cell data on cell-type and receptor subtype selectivity suggest raloxifene can show a fairly distinct pattern across receptor subtypes and human cell lines. That helps explain why it behaves so differently from the old triphenylethylene compounds.
Still, you do not want to get seduced by receptor-subtype trivia and miss the practical point. PCT is not won by saying "this one likes ER beta more." It is won by solving the actual problem in front of you. If the issue is suppressed gonadotropins, central feedback matters more than elegant receptor trivia. If the issue is breast tissue stimulation, tissue antagonism in the breast matters more.
Same receptor family. Different battlefield.
Coregulator shift
This is the hidden lever. The receptor is only half the machine.
Once a SERM binds, the receptor changes shape and starts attracting either coactivators or corepressors. Those helper proteins differ by tissue. That is why one drug can support bone while opposing breast growth, or block one promoter while allowing another to fire.
Research on coregulator abundance and tissue selectivity makes this pretty clear. Tissue context changes the output. You are not dealing with a simple on-off switch. You are dealing with a drug-receptor-coregulator complex that behaves one way in one cell and another way in the next.
For post-cycle readers, the takeaway is brutally simple: do not treat "SERM" like a single category with a single effect. That is like calling boxing, wrestling, and fencing "sports" and acting shocked when they produce different bruises.
Structural features
Chemistry is destiny more often than people want to admit.
The reason clomiphene, enclomiphene, and raloxifene do not behave the same way is not just branding, not just dose, not just who wrote the forum post. Their structures are different enough to produce different receptor conformations and different downstream effects.
Triphenylethylene scaffold
Clomiphene belongs to the old triphenylethylene family, the same broad structural world that includes tamoxifen. These are nonsteroidal synthetic ligands with a bulky aromatic system and a side chain that interferes with the clean receptor closure you get with estradiol.
Estradiol is compact and steroidal. Clomiphene is not. That matters.
The triphenylethylene scaffold gives you flexibility, but also a kind of messiness. The receptor complex can land in a partly antagonistic, partly agonistic state depending on tissue, promoter context, and local coregulators. In ER alpha, residues such as Asp 351 are part of the chemistry discussion around how these ligands stabilize antagonistic versus partial-agonist states, though the exact behavior varies by compound.
That older scaffold is powerful. It is also a little blunt.
Clomiphene works, but it works like an older tool works. Effective, yes. Elegant, not always.
Benzothiophene scaffold
Raloxifene sits in the benzothiophene class, and that difference is not cosmetic. Its scaffold is more rigid, and it tends to produce a receptor conformation that is less permissive to uterine stimulation than older SERMs.
That is one reason raloxifene looks safer for the endometrium than tamoxifen and why it became important in bone-focused and breast-risk settings. The old dream with newer SERM design was simple enough: keep the good estrogen effects where you want them, especially bone, and strip out the bad ones where you do not, especially the uterus and breast.
Nobody achieves perfection. Still, raloxifene is much closer to that design goal than clomiphene.
It also has quirks of its own. As work on metabolic pathways and glucuronidation-driven availability notes, raloxifene undergoes heavy first-pass metabolism and extensive glucuronidation. So even before you get to tissue effects, you are already in a different pharmacology universe.
Isomer effects
If you remember only one chemistry fact from this whole article, make it this one: enclomiphene is not just "another name" for clomiphene.
Clomiphene is a blend. Enclomiphene is the isolated trans isomer from that blend.
Why do people care? Because the trans isomer appears to carry more of the hypothalamic-pituitary antiestrogenic action that raises LH and FSH, while zuclomiphene contributes more lingering estrogenic drag. That lingering part is not trivial. Zuclomiphene has a longer effective tail, and that can make clomiphene feel less clean over time.
This is why many people describe enclomiphene as a more targeted recovery tool. Not magic. Not side-effect-free. Just more aligned with the actual post-cycle goal.
Tissue effects by drug
This is where the abstract receptor talk cashes out in real life.
You do not feel a ligand-binding domain. You feel libido, mood, nipple sensitivity, joint comfort, erections, sleep, maybe a strange visual disturbance, maybe a hot flash that feels absurd because you did not think that was your demographic. Tissue effects are the story.
Hypothalamus
For PCT, the hypothalamus is the front gate.
Clomiphene and enclomiphene both matter here because they reduce estrogenic feedback at the hypothalamus and pituitary. That can increase GnRH pulsatility upstream and then LH and FSH downstream. If your testes still have capacity to respond, testosterone can rise.
This is exactly why these two keep showing up in post-cycle conversations. They target the signaling choke point.
Enclomiphene often gets the nod when someone wants the cleaner version of that effect. Clomiphene is more established and more widely known, but it drags its isomer baggage behind it. Whether that difference becomes clinically huge for you is a separate question. Some people tolerate clomiphene just fine. Others hate how they feel on it. Endocrine drugs are like that. They are annoyingly personal.
Raloxifene is simply less convincing here as a primary "wake the axis back up" choice. It can interact with estrogen signaling, obviously, but if your main target is gonadotropin recovery, it is usually not the first name on the list.
Breast and uterus
Breast tissue is where raloxifene starts making more intuitive sense.
It behaves as an estrogen antagonist in breast tissue, which is why it has long been valuable outside PCT discussions. In a post-cycle setting, if someone is worried about gynecomastia or active nipple flare-ups, raloxifene gets attention because of this profile.
Clomiphene and enclomiphene are not pointless here, but breast tissue control is not their cleanest selling point. Their main value is still central feedback, not direct breast-focused selectivity.
Now the uterus. For many PCT readers this is not personally relevant, but it matters scientifically because uterine behavior is one of the classic ways SERM selectivity is measured.
Raloxifene is generally antagonistic or close to neutral in the uterine endometrium, which is one reason it is often contrasted with tamoxifen. The STAR trial's comparative adverse profiles are part of why clinicians grew comfortable saying raloxifene brings less uterine baggage than older SERM options.
Clomiphene is different. In women, it can behave in antiestrogenic ways at the endometrium and cervical mucus even while it stimulates ovulation through the brain. That odd split is pure SERM logic. One tissue sees blockade, another tissue sees the endocrine ripple effect from rising gonadotropins. This is also why clomiphene is useful in fertility medicine and annoying in fertility medicine, sometimes at the exact same time.
Bone and liver
Raloxifene clearly wins the bone conversation.
Its estrogen-like action in bone is not theoretical fluff. Trials such as the MORE study on vertebral fracture and bone density outcomes showed the kind of bone preservation that built its clinical identity. If you are comparing tissue effects across the three drugs, this is one of the cleanest distinctions on the page.
Clomiphene and enclomiphene do not occupy that role. They may indirectly help bone health in men if they restore testosterone and allow a healthier estradiol range, because bone needs estrogen too, but that is not the same as being a dedicated bone SERM with outcome data.
The liver is trickier. SERMs can improve some lipid markers, but they also influence coagulation pathways. That means you cannot glance at a cholesterol panel and declare victory. Raloxifene, in particular, carries a real venous thromboembolism concern. Clomiphene is not exempt from clot risk either, even if it is discussed more casually in men's health spaces than it should be.
A second table helps make the tissue split less fuzzy:
|
Tissue |
Clomiphene |
Enclomiphene |
Raloxifene |
|---|---|---|---|
|
Hypothalamus / pituitary |
Strong practical relevance for raising LH and FSH |
Strongest conceptual fit of the three for this purpose |
Less central evidence for primary restart use |
|
Breast |
Mixed value, not primarily chosen for direct tissue selectivity |
Similar story, still not the main reason to choose it |
Stronger antagonist profile, often discussed for gyno-related concerns |
|
Uterus / endometrium |
Mixed and context-dependent in women |
Less defined clinically than clomiphene |
Generally antagonistic or neutral, lower uterine stimulation than older SERMs |
|
Bone |
No major direct clinical identity here |
Same |
Clear agonist-like benefit, established osteoporosis role |
|
Liver / coagulation |
Hepatic metabolism, rare but real clot concerns |
Similar class caution, less long-run history |
Known clot risk, strong hepatic handling through glucuronidation |
Generation and pharmacology
Drug generations are useful until people force them too hard.
Older agents
Clomiphene is old-school. It came from an earlier era of SERM development, closer in spirit to tamoxifen than to the newer breast-bone-uterus balancing act that drove second- and third-generation design.
That does not make it bad. It makes it broad and somewhat blunt.
Older agents often have a bigger historical footprint and more messy real-world experience. You know what they tend to do, but you also know the tradeoffs are not especially refined.
Newer selectivity
Raloxifene is generally classed as a second-generation SERM. It was built to keep antiestrogenic effects in breast tissue, protect bone, and avoid the uterine stimulation that plagued older molecules. In that specific design sense, it is the more selective, more modern drug.
Enclomiphene is a little different. It is not usually discussed as "third-generation" in the classic way bazedoxifene might be. It is better understood as a purified active isomer strategy. Same family roots as clomiphene, but narrowed down to the isomer you actually wanted for male endocrine signaling.
That is a smart move, honestly. Rather than invent a whole new receptor story, strip out the part that muddies the one you already have.
Active metabolites
People love to assume every SERM works like tamoxifen, where active metabolites such as endoxifen matter enormously. That assumption causes more confusion than clarity.
Clomiphene is not mainly a "wait for one magic metabolite" story. Its behavior is strongly shaped by the parent isomer mix itself, especially the enclomiphene versus zuclomiphene split. Enclomiphene as a standalone agent avoids much of that built-in pharmacologic clutter.
Raloxifene is different again. Its oral pharmacology is dominated by extensive first-pass handling and conjugation rather than a famous single active metabolite narrative. So when people say "all SERMs are basically the same after the liver gets them," no, not really.
Pharmacology remains stubbornly specific.
Which option fits post-cycle goals?
This is where people want a clean winner. Life would be nicer if there were one.
There usually is not. There is just a better fit for the problem you actually have.
LH and FSH support
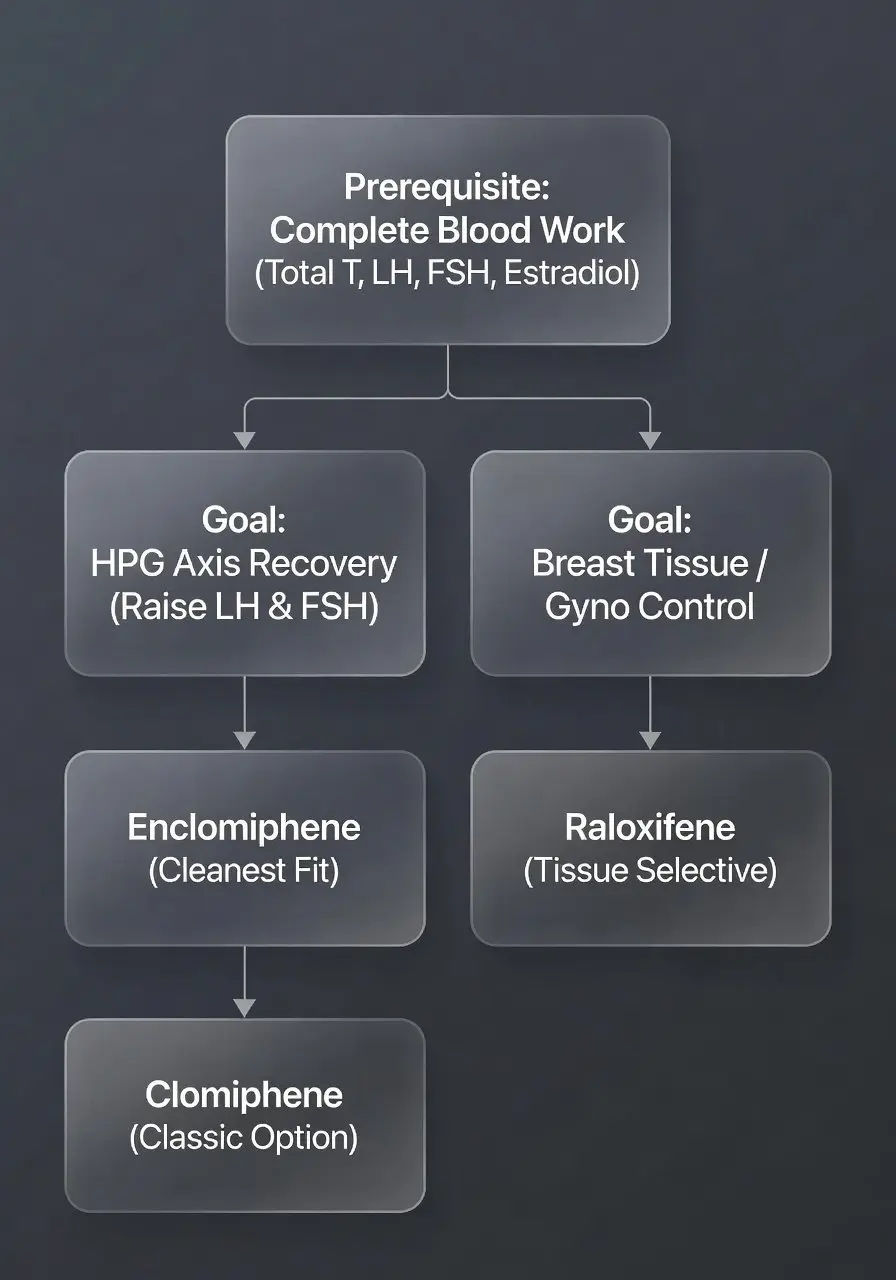
If your real goal is to nudge the HPG axis back into motion, enclomiphene is the most purpose-aligned of the three, and clomiphene is the most familiar practical option. Both work by easing estrogenic negative feedback at the hypothalamus and pituitary, which can raise LH and FSH and, in turn, testosterone.
Raloxifene sits behind them for this goal.
That does not mean raloxifene is useless. It means it is not usually the most direct tool if your labs show suppressed gonadotropins and you are trying to restore endogenous production.
And a small reality check belongs here. Post-cycle drug use should be a targeted tool, not a ritual. If your blood work is recovering, symptoms are mild, and you are not dealing with fertility issues or prolonged suppression, you do not automatically need to throw medication at the problem because the internet acts like abstaining is failure. Anti-guilt-trip medicine is a decent rule in endocrine land.
Estrogen symptom control
This part gets butchered online.
A SERM can block estrogenic action in some tissues without lowering total estradiol. So if you are puffy, emotional, hypertensive, and aromatizing hard, a SERM may only solve part of the problem. It may help breast tissue while doing very little for water retention or the general "high estrogen" feel.
That is why the question cannot just be "Which SERM is strongest?" You have to ask what symptom you are even trying to control.
If the concern is nipple sensitivity or glandular breast changes, raloxifene may deserve a hard look because its breast antagonism is a more natural fit.
If the concern is crashed LH, FSH, and testosterone after suppression, clomiphene or enclomiphene are the more rational first thoughts.
If the concern is "I feel weird," be careful. Not every rough post-cycle week is an estrogen receptor problem. Sleep debt, low calories, low fat intake, dehydration, anemia, thyroid issues, and plain old withdrawal from supraphysiologic androgen exposure can all wear the same mask.
When tradeoffs matter
This is usually the real decision point:
-
If fertility and testicular function are the center of the conversation, clomiphene or enclomiphene usually make more sense than raloxifene.
-
If active breast tissue symptoms are the center of the conversation, raloxifene may line up better with the tissue problem.
-
If you have a history of visual issues, mood instability, or clot risk, the choice gets narrower fast.
-
If your labs are incomplete, you are guessing, and guessing with endocrine drugs is how people create new problems while trying to fix old ones.
That last one deserves a glare. People obsess over molecule choice while flying blind on total testosterone, free testosterone, LH, FSH, estradiol, prolactin, SHBG, and sometimes semen parameters if fertility is a goal. That is backwards.
Side effect patterns and limits

No SERM is "clean." Some are simply cleaner for a particular job.
Clomiphene is famous for a reason. It works often enough to stay in the conversation, but it can bring visual disturbances, mood swings, headaches, nausea, and the occasional odd sense that your hormones are technically improving while you feel emotionally off. I suspect some of that reputation comes from the mixed-isomer nature of the drug, though side effects are never as tidy as one theory.
Enclomiphene should, in principle, avoid some of the noise created by zuclomiphene. That is part of the appeal. Still, "should" is not the same as "guaranteed." The data set in young men using it broadly and long term is not as deep as the internet sometimes pretends.
Raloxifene has its own pattern. Hot flashes, leg cramps, and clot risk are the headliners. In the wrong person, that clot issue is not a side note. It is the whole conversation. The same goes for stroke risk in susceptible groups. A drug can be elegant at the receptor and still be a bad fit for your body.
A few practical patterns are worth keeping in one place:
-
Clomiphene often gets chosen because it is available and familiar, but it may feel less predictable because of its isomer mix.
-
Enclomiphene looks cleaner for central recovery goals, though access and long-run evidence can be limiting.
-
Raloxifene looks more attractive when breast tissue selectivity matters, but it is usually a weaker answer for restarting LH and FSH.
-
All three can disappoint you if the real issue is not estrogen signaling in the first place.
That last point matters more than people admit. Sometimes post-cycle fatigue is not from a mystical blocker, not from some exotic receptor failure, just from bad inputs. Too little food. Poor sleep. Low micronutrient intake. Overreaching in the gym while your endocrine system is already trying to relearn normal. Boring causes still count.
What should you ask before choosing?
The best question is not "Which one is best?"
The best question is "Best for what, exactly?"
Ask yourself, and preferably your clinician, a few things before you get cute with receptor pharmacology:
-
Is your main goal testosterone recovery, fertility preservation, or breast symptom control?
-
Do you have actual labs showing low LH and FSH, or are you reacting to how you feel?
-
Have you had clotting issues, migraines with visual aura, retinal problems, or major mood swings before?
-
Are you expecting a SERM to lower estradiol, even though that is not what it mainly does?
-
Are you treating a real post-cycle problem, or following a ritual because forums made it sound mandatory?
That last question stings a little. Good. It should.
FAQ
Is enclomiphene just clomiphene with a different label?
No. Enclomiphene is the trans isomer isolated from clomiphene. Clomiphene contains enclomiphene plus zuclomiphene. That difference matters because the isomer mix changes pharmacology, duration, and likely side-effect feel.
Does raloxifene raise testosterone the same way clomiphene does?
Not usually in the same practical sense. Clomiphene and enclomiphene are much more directly tied to raising LH and FSH by reducing estrogen feedback at the hypothalamus and pituitary. Raloxifene is more valued for tissue-selective antagonism, especially in breast tissue, and for bone effects.
Do these drugs lower estrogen levels?
Not directly. They are selective estrogen receptor modulators, not aromatase inhibitors. Your estradiol level can remain similar while receptor signaling changes in specific tissues.
Which one makes the most sense for gynecomastia concerns during PCT?
Raloxifene often enters the discussion because of its breast tissue antagonism. That said, established gynecomastia, early nipple sensitivity, and plain fat gain are not the same thing, and people confuse them constantly. Timing and diagnosis matter.
Which one makes the most sense if your goal is LH and FSH recovery?
Enclomiphene is the cleanest fit conceptually. Clomiphene is the classic real-world option. Raloxifene usually trails both for that specific purpose.
Are side effects usually milder with enclomiphene than clomiphene?
They may be, at least in theory, because you are removing zuclomiphene from the picture. But "may" is the honest word. Individual response still runs the show, and the evidence base is not as mature as clomiphene's longer clinical history.
Can you use a SERM for PCT without blood work?
You can. People do. That does not make it smart. Without labs, you are guessing whether the problem is suppression, estradiol-related symptoms, prolactin, poor recovery habits, or something else entirely.
Conclusion
The lazy take is that clomiphene, enclomiphene, and raloxifene are all just SERMs, so you can swap them around like batteries.
You cannot.
Clomiphene is the old, familiar, mixed-isomer workhorse.
Enclomiphene is the sharper version aimed more cleanly at LH and FSH recovery.
Raloxifene is the more tissue-selective outlier, stronger on breast and bone logic than on central restart logic.
So if you are looking at PCT through the lens of actual mechanism, the split is pretty plain. For axis recovery, the clomiphene side of the family makes more sense. For breast-focused estrogen symptoms, raloxifene can make more sense. For long-term health and side effects, none of them deserve casual treatment.
Pick the drug for the problem you actually have. Not the one the loudest guy in the forum swears by.
Articles

GH stands for growth hormone, a hormone produced by the pituitary gland that plays a key role in growth, recovery, metabolism, and hormone regulation. This guide explains GH medical terminology, HGH therapy terms, and the most important growth hormone definitions used in medicine and bodybuilding.

So you have decided to embark upon your very first adventure known as a prohormone cycle! Without a doubt, you are going to enjoy the results that you are about to see.

BPC-157, TB-500, and CJC-1295 are popular recovery peptides used for tissue repair, healing support, and growth hormone optimization. This guide explains how these peptides work, compares their evidence and mechanisms, and explores potential benefits, risks, and safety considerations.
Customers Reviews
Please leave your review on products or service below.
Thank you beforehand.